
From my clinic:
Mrs Mulyani visited my clinic, with her husband, who sufferred hearing difficulty.
Her husband, 39 years old, conducted right ear mastoidectomy on 2003 . Three months ago, left ear worsened. They brought recommendation from an ENT specialist.
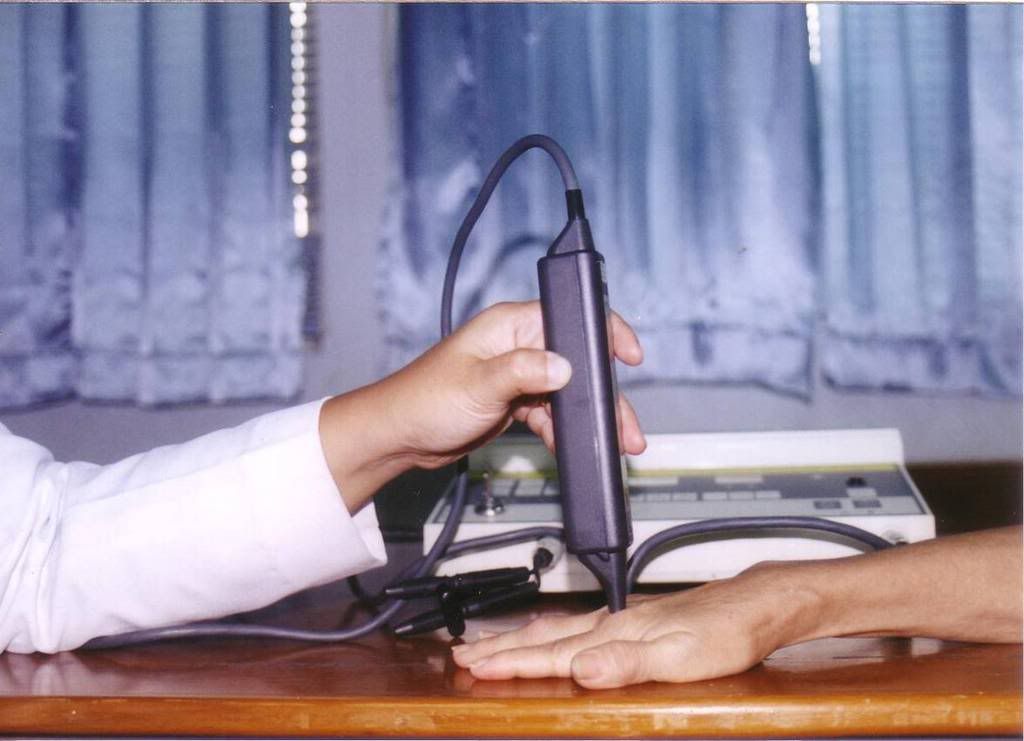
He complaint headache , noisy both ear, poor balance while walking. Low power laser given by ILIB and ear approach, ones a week, for 10 times. ILIB with opening 50 %, for 1 hour, and ear with 650 nm Low laser , 10 mW, 1 hour, pulse, for both ear. Probe approach given ones, at 9th visit, for neck spasm.

After 4th visite , could hear his son crying and adzan from mosque. .
After 5th, pain killer minimize , muscle relaxant stop .
After 6 visite, could speak with normal pitch, balance going better. No headache anymore.
rare,almost disappear.
Program: going to administer 10 times again, ILIB ,and ear.
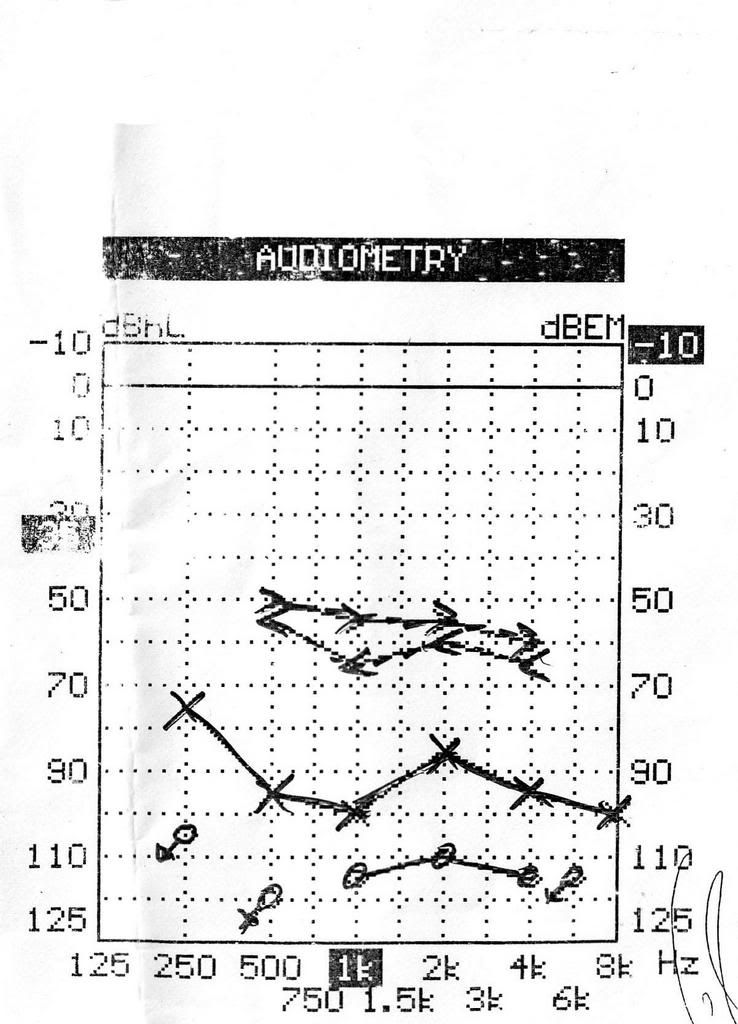
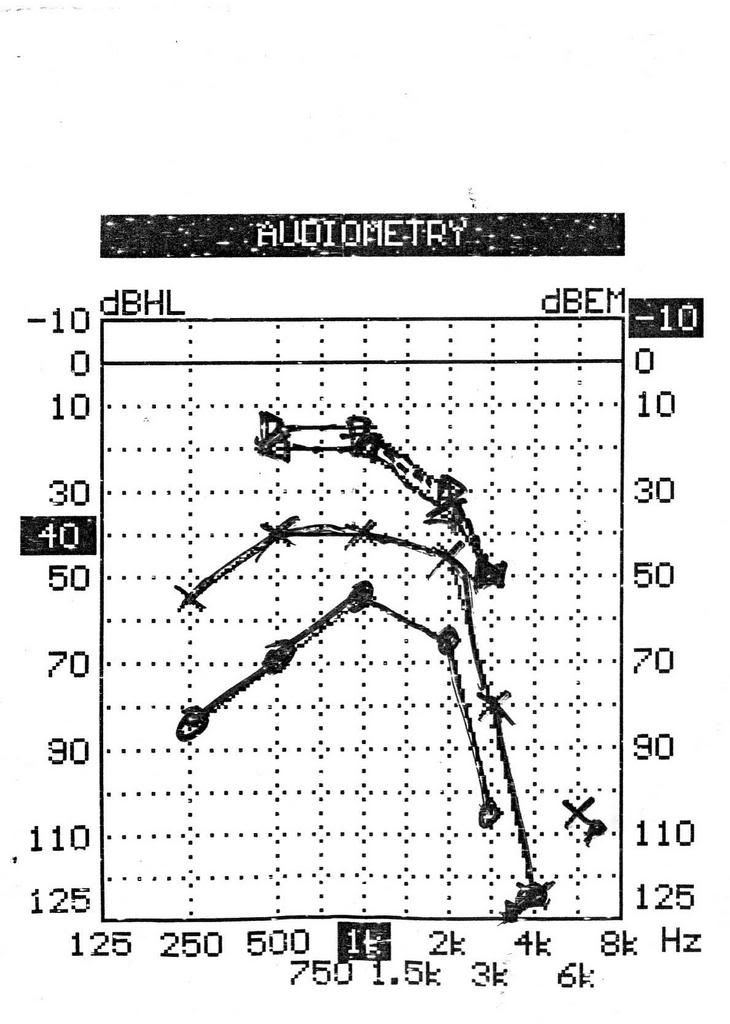
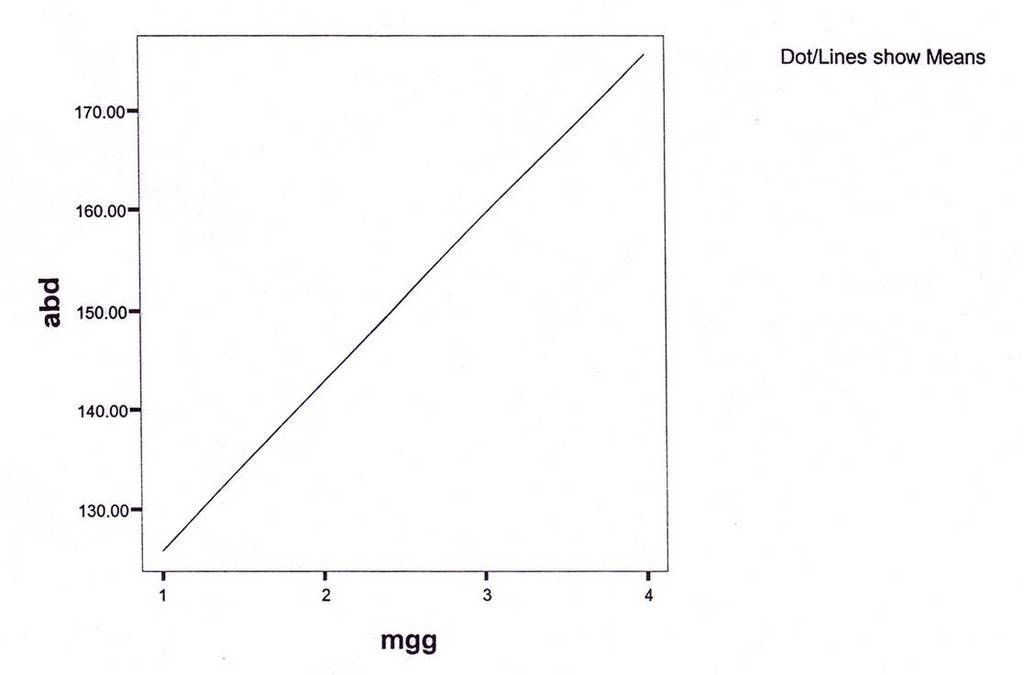
Audimetry: going better compare before LLLT.(Before 5 January 2007 - left diagram, After, 20 March 2007 ; right diagram)
Left : April 4, 2006 ; Right : April, 25, 2006
riht ear: increas 39 dB[ left ear increase : 19 dB
Discussion:
Balance maintance by hearing, visual , and proprioceptive. No doubt he complaint poor balance while walking. To maintain balance, he try to stabilize the neck, so muscles of the neck became stiff.
Balance , and neck muscle pain became better as well as the hearing.
I surprised, he answered my call by cell phone, after 14th therapy.
no pain killer , and muscle relaxant anymore. Tinnitus, gone.
Some journals said , LLLT not work for tinnitus.
May be the dose is to small as well as my experience before I use ILIB , and ear probe.
He is going to work again
From journals:
The low level laser therapy of inner ear diseases has been made use of in Germany since the end of the eighties (for example by Dr. Uwe Witt, Hamburg) and is also to be found in quite a few other countries (Italy, France, Scandinavia, Switzerland, Hungary, the United States of America, Russia etc.).
Since 1991, about 800 inner ear patients have been treated with low level laser light under the medical and scientifical supervision of me. The therapy results have been (and still are) continuously documented and analyzed
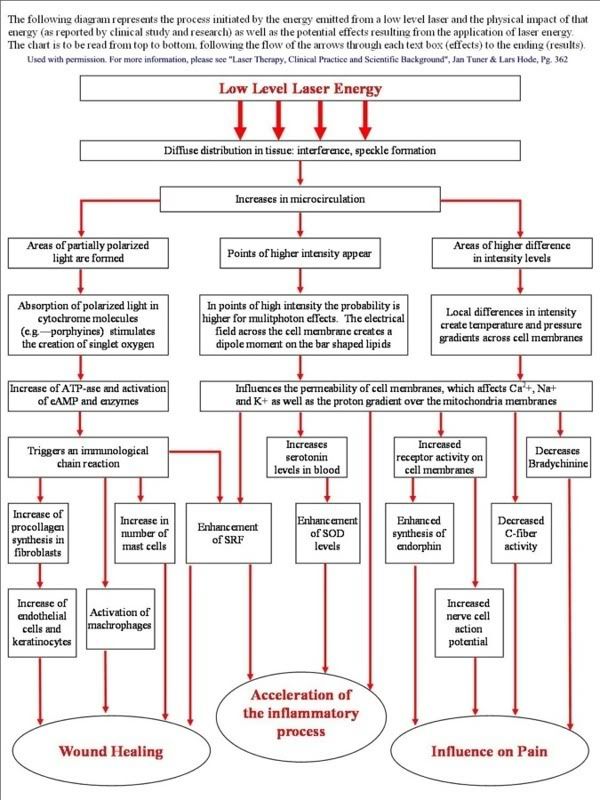
How does LLLT work?
Each cell contains a number of power plants, called mitochondria. The function of these power plants is to produce ATP, the form of energy which can be used by the cell to function properly.
The inner mitochondrial membrane is a large collector surface folded onto a small total volume. All nutritive molecules (fats, proteins and glucose) are oxidized within the cell to the last molecular nutritive component, that is, pyruvate. The pyruvate is then imported into the cellular power plant, where it disintegrates into carbon dioxide and water in the immediate proximity of the collector surface of the mitochondrion. The molecular bond energy thus released, which corresponds with visible, ultraviolet and infrared light as far as its wavelength and frequency is concerned, is utilized by the mitochondrion to produce the cellular fuel ATP.
The collector surface of our cellular power plant is enlarged by the mushroom-shaped protrusions of the inner mitochondrial membrane. The molecular bond energy of the pyruvate is released in the form of light energy. The antennae pigments are capable of absorbing this light energy and transmit it to our cellular power plant, which can now produce the cellular fuel ATP. The natural solar radiation also stimulates the antennae pigments of the mitochondrion to produce ATP.
The cellular power plants can thus produce more ATP. The cellular energy is the fuel the inner ear cells strives after and needs. A sufficiently high supply of cellular energy enables our inner ear cell to work under optimum conditions and is the essential prerequisite to ensure a successful self-healing process.
Low level laser light increases the energy output in our cellular power plant.
(For a detailed discussion, see article: Import of Radiation Phenomena of Electrons and Therapeutic Low-Level Laser in Regard to the Mitochondrial Energy Transfer, Journal of Clinical Laser Medicine & Surgery, Volume 16, Number 3, 1998, Mary Ann Liebert, Inc., Pp.159-165 )
Balance:
Is it possible to help the organ of balance with the high dosage low level lasertherapy by Dr. Wilden¨, specialist of Morbus Menière treatment?
Yes. Vertigo, Morbus Menière and the often in the same time existing sensation of pressure in or surround the ear can be treated very well with the high dosage low level lasertherapy by Dr. Wilden¨, specialist of Morbus Menière treatment.
* from "Das Stato-Akustische Organ" / Reiss-Walkowiak-Zenner-Plinkert-Lehnhardt





























{kind=link}