Mr Ernando , sent to me by dr Sutji, a neurologist, due to severe pain. She asked me to make rehabilitation program.
I asked him to stay in hospital, to seek which management could control the pain, and to make othose to make his right arm still useable.
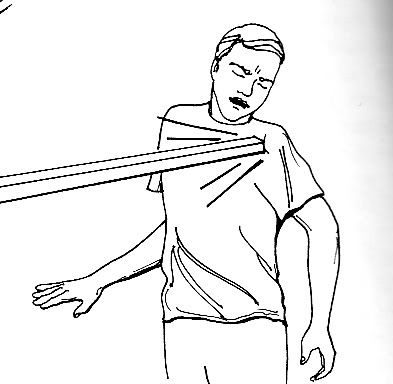
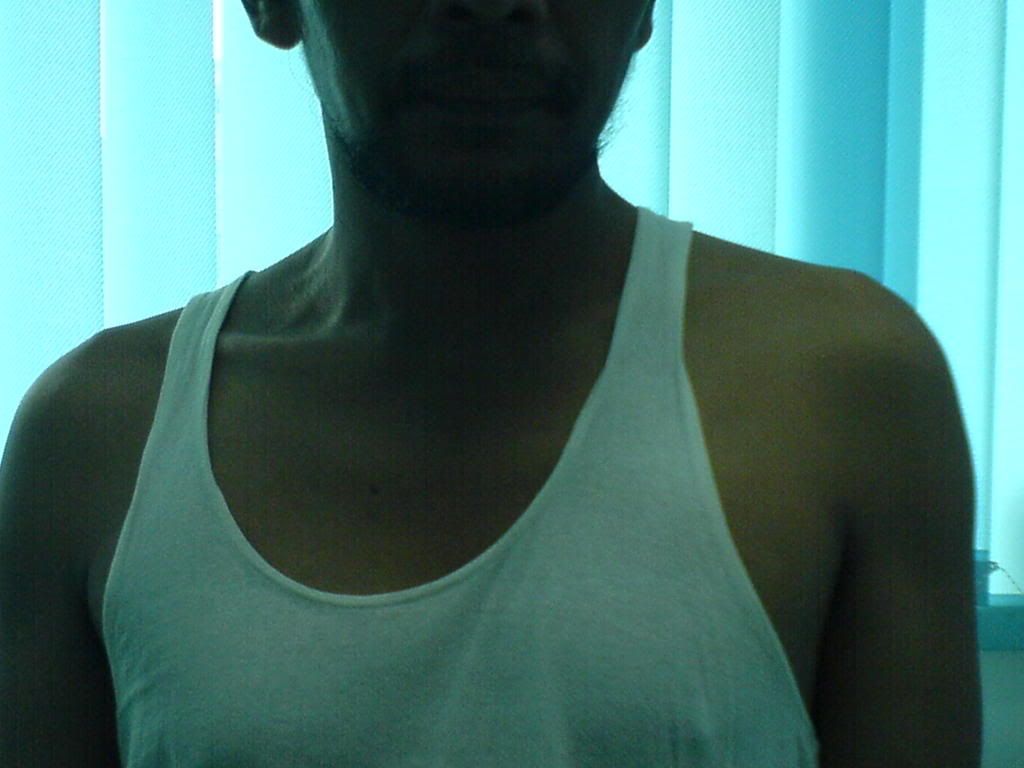
It was important to manage the pain, due to bad posture he maintained .He walked in my office with his head tend slight bend to the right , position he used after injury to reduce the pain. If he could maintain the pain, he would able to control his posture, and could use his right hand. As the result, it helps to diminishes the atropy of the muscle. You could see, his right shoulder lower than his left side.
Mr Ernando work at mining corporate, he usually work down the earth. He and his friends us small train as the mobility devise. The inury happened when the train slipped, and his shoulder hit by hard stone.
Shoulder joint (= glenohumeral joint)
Shoulder joint , is a joint between glenoidales and humerus, so we could name it by glenohumeral . Glenohumeral joint is prone to dislocation due to its relatively poor bony fit and limited supporting musculature. The shallowness of the glenoid fossa and limited contact area between the fossa and the humeral head contribute to the joint instability .
In normal (undamaged capsule ) glenohumeral joint, a small negative intracapsular pressure helps stabilize the joint.
He brought roentgen taken after the injury, and the result was it was posterior dislocation.
Posterior dislocation was results from anterior direct trauma . (Biomechanics of musculoskeletal injury, William C Whiting; Ronald F zernicke; Human Kinetics, 1998)
Discussion:
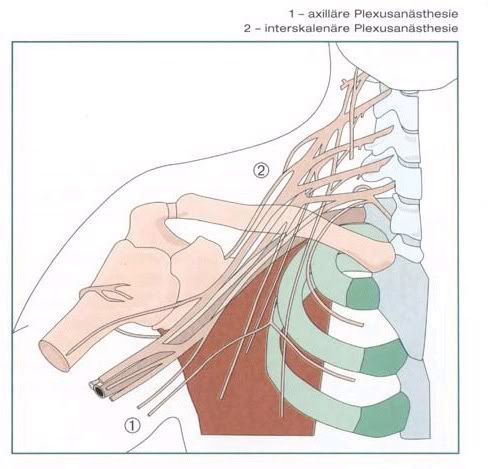
When he came on May 8, 2007, I found deficit sensory 40 % - 60 %. Yes, injury at shoulder site, also could damage the brachial plexus. EMG taken before explained the deficit .
Hospitalized a week, given medicine for pain, drink by the clock; infra red radiation and electrical stimulation; exercise for correction his posture , and prevent further athropy.
Discharge from hospital with toradol 4 times daily, correct posture. Could used right for activity daily living. I asked him to use arm sling and shoulder sling simultaneously. Three times a day exercise to prevent atrophy, take the pain killer by the clock.
I wrote report to his doctor, a general practitioner as host doctor, and suggest if he could work not in the hole down the earth for few weeks. The doctor recommended to work behind the desk at head office,
Visited for control, May, 28 – 2007, deficit sensory 20 % .
A month later, I recommended him to work at the mining . He is an expert at explotion division. I asked him to use both hand to set the little bomb.
Although it is a good case for low laser, it was not suitable for him. He must back to work again , in the middle of the forest. , as soon as possible. If he stay at home, or stay in Jakarta to take laser , he just get the basic salary. The best income, if he do the exp lotion again.
As a doctor, especially a physical medicine and rehabilitation specialist ,we must take that as a consider. A team must build, with other doctor , therapist and social worker as needed.
Others drugs given as needed, like neurotropic agent , to help nerve repair.
We will follow by EMG , 3 month after the first one
Any comment ?