 This week I share two cases of mine. Ankle sprains and osteoartritis genu.
This week I share two cases of mine. Ankle sprains and osteoartritis genu.Story from my clinic
Mrs Dianiati a lady pulmonologyst from a famous hospital in
It was so painful, she could not rise immediately. For few minutes she seated on the floor , her lower extremity, below the knee, began edema suddenly.
Roentgen took the day after (Tuesday), bony intack, so the diagnose was ankle sprain. I asked her to visit my clinic, laser administered, diode laser 90 mW; 12 J/cm2 , with probe mode , totally 10 points.
I met her on Wednesday at Cipto Mangunkusumo, edema was gone, just swollen around her ankle. Mobility independently, used sandals, one crutch as cane, but the pain still annoying. Saturday afternoon (3rd March 2007), I gave her diode again but this time for her pain.
(I wrote this report Sunday, 4th oh March 2007.)
Discussion : At her first visited , the laser given to relive the edema, and second visit for the pain.
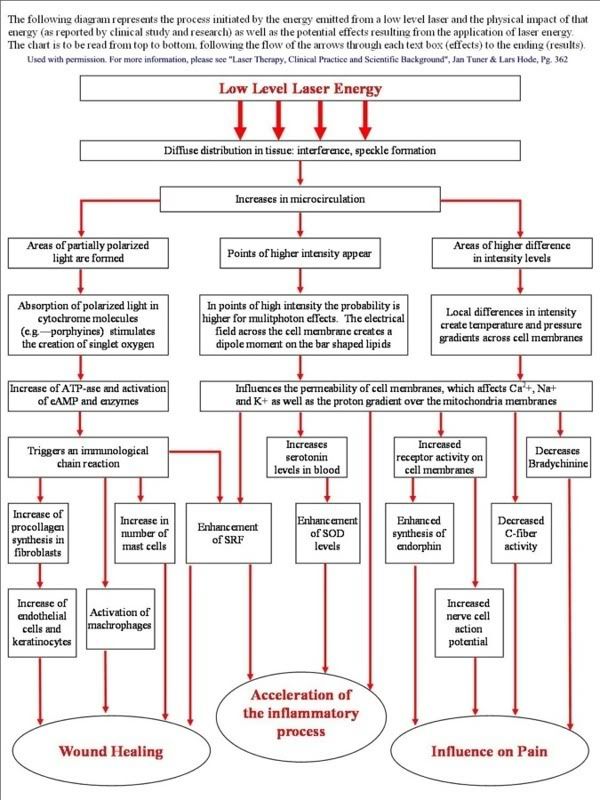
Ussually the recovery will take four weeks, but at the first week, she already ambulation with minimal dependent. Edema decrease because effect emitted energy laser to the microcirculation, and influenced on pain due to effect to the C-fiber activity and bradychinine. (I enclose diagram represent the proces initiated by the energy emitted). The dose and the mode the laser delivery take important place to get best result. It is a therapeutic window must be understand, and also the mode to reach the site of the damage.
Low-level laser therapy in ankle sprains as randomized clinical trial
OBJECTIVE : The test the efficacy of low-level laser therapy on lateral ankle sprains as an adition to standardized treatment regiment, a trial was conducted in which high laser (5 J/ cm2), low-dose laser (0.5/cm2),and placebo laser therapy (0J/cm2) att skin laser level were compared .
DESIGN: Randomized , double-blind, controlled clinical trial with a follow-up of 1 year. Patients, therapist, assessors, and analyst were blinded to the assigned treatment.
SETTING: An ambulatory care setting.
PATIENTS: After informed consent and verification of exclusion criteria, 217 patients with acute lateral ankle srains were randomized to three groups from September 1, 1993 , through Desember 31, 1995.
INERVENTIOS: Twelve treatments of 904 nm laser therapy in 4 weeks as an adjunct to a standardized treatment regiment of 4 weeks of brace therapy combined ith standardized home exercise and edvice. The laser therapy device used was a Ga- As laser , with 25-watt peak power and 5,0000 or 500 Hz frequency, a pulse duration of 200nsec, and an irradiated area of 1cm2.
PRIMARY OUTCOME MEASURES : Pain and function as reported by the patient
RESULTS: Intervention –to- treat analysis of the short term results showed no statistically significant difference on the primary outcome measure, pain (p=.02) and at some points for hindrancein activities in daily life and pressere pain, as well as subjective recovery (p+.05). intention-to-treat analysis showed that total days absenteeism from work and sports were remarkably lower in the placebo group than in the laser groups, rangimg from 3.7 to 5.3 and 5 to 8 days, respectively. The total number of relapsesat 1 year in the low-dose laser group (n=22) was significantly higher (p=.04) than in the other two groups (high laser, n=13; placebo, n=13). Subgroup analysis to correct for possible confounders did not alter these findings.
CONCLUSIONS: Neither high- nor low dose laser therapy is effective in the treatment of lateral ankle sprains.
Arch Phys Med Rehabil. 1998 Nov;79(11):1415-20







