Going next reports for you.

Mrs Nurati. Long case neuropathy
ILIB for stroke

LLLT for sinusitis

LLLT for dysphagis

LLLT for hipokalemi

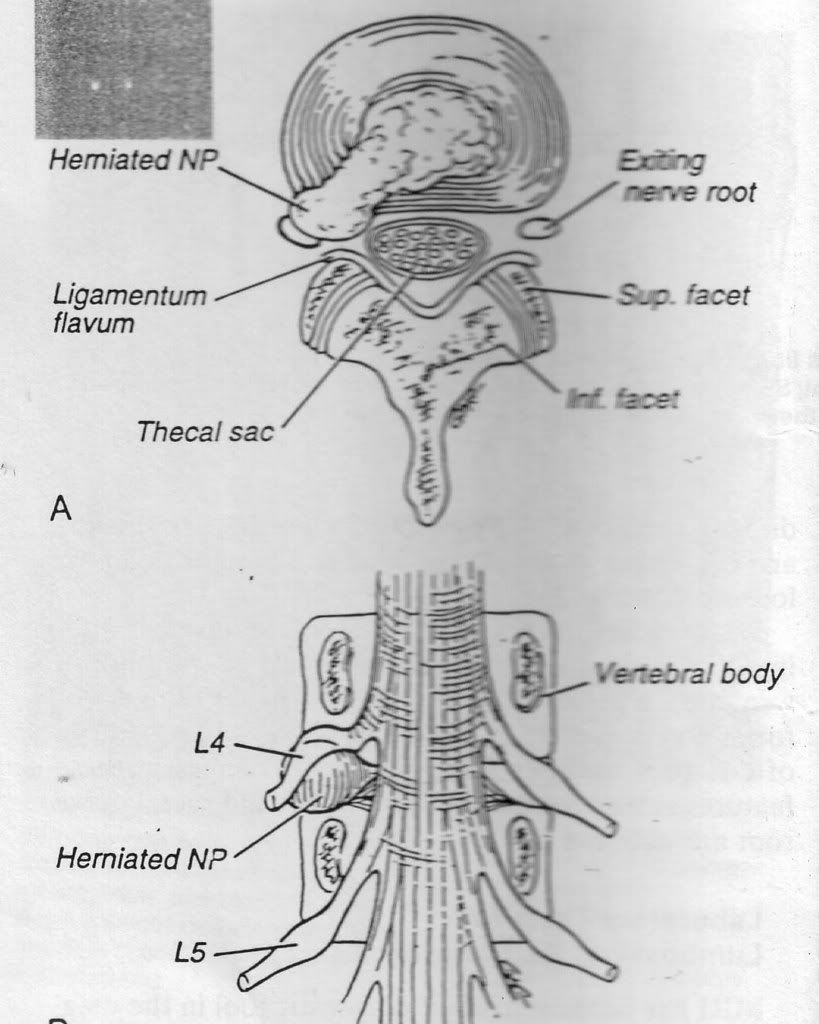
Yes, Sir. Your problem is common to middle-age man, especially after strenuous activity. You did gardening, and pulled bushes . Your roentgens shows bulging at L2. 3.4 and 5. the pain radiated to your buttock, posterior thigh , and lateral calf. It follows the path of sciatic nerve .

Therapy began with totally bed rest due to your pain (vas almost 10). Modality TENS to reduce the spasm. But after almost 3 weeks, your pain still above 6, laser is the answer. First with transcutaneus approach, 30 minutes. The pain still annoying, although you could ambulation using lumbosacral corset and cane. It was comfort for your at 1 hours therapy .
So , I decided to used ILIB, given twice a week. The pain gone after the 4th ILIB, walking freely , erect , without cane, after 5th therapy, and your daily activity full recovery. (You do gardening and riding your motorcycle).
Discussion:
Along with laser ubi quinon , and neurotropic agent . Ubi quinon works at mitochondria as well as the laser. Neutropic agent for nerve healing conjunctions with laser.
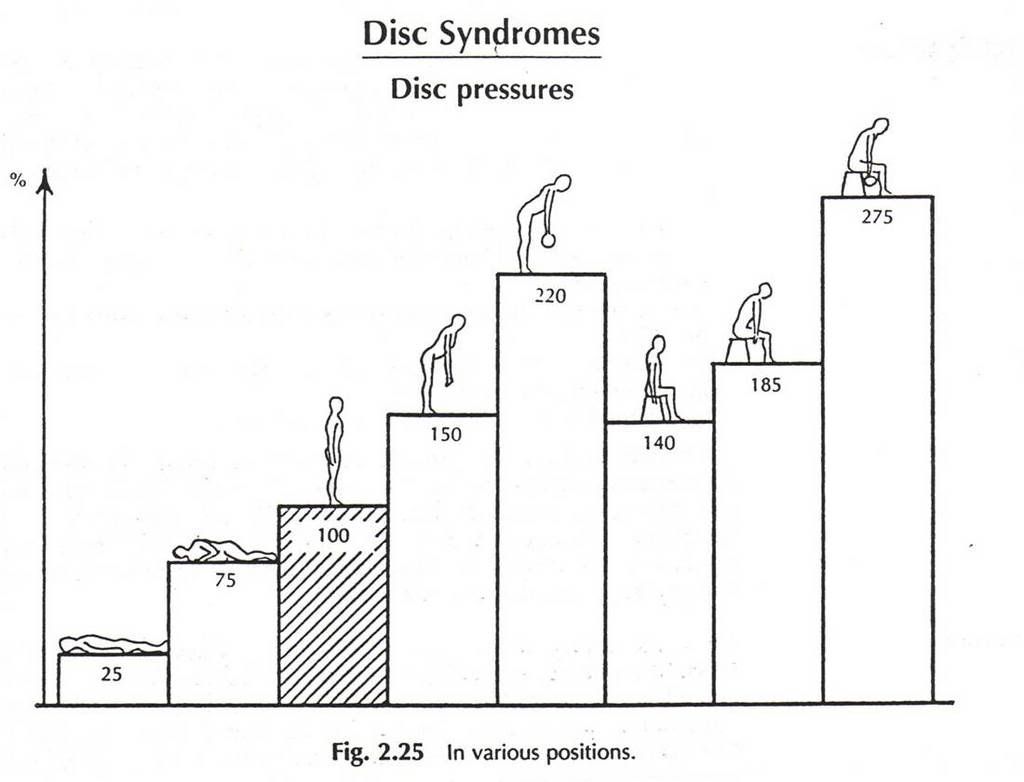
Figure above demonstrates relative changes in L3 disk pressures in various position . Although in lying position, no weight free. In patient with HNP, lumbosacral orthose reduces or avoid weight , so no nerve impingement .
ILIB more forceful than transcutaneus. As the results, your pain reduced faster.

by Andrei P. Sommer Department of Biomaterials, ENSOMA-LaCentral Institute of Biomedical Engineering
| ||
| |
Wound healing via laser light goes back to Prof. Endre Mester. First reports on his pioneering work started in 1967. For biostimulation he used the coherent light of powerful 50mW He/Ne-lasers (632.8nm). The Mester group has been continuously successful from the beginning. But only a minority of researchers could reproduce the success of the biostimulation experiments. 33 years after introducing the paradigm of photobiostimulation, the LILAB-equation has been anchored into LLLT [1] - establishing the biological limits of the dose (energy density) and the light intensity. Recent laboratory experiments, demonstrating that various individually administered wavelengths of laser light applied at energy densities of the same order induced comparable biological effects in rats, could be interpreted as additional evidence in support of the LILAB-equation [2].
During the 1st NOA Conference [3] a multidisciplinary group of ten scientists from Brazil, Denmark, Finland, France, Germany, Hungary, Israel, Saudi Arabia and U.S.A. evaluated possibilities of validating LLLT. One of the discussed visions has been to directly investigate the molecular mechanisms of light-induced wound healing processes occurring in LLLT via Nearfield Optical Analysis (NOA). The vision has been so promising that Attila Pavláth - President ACS - became eventually interested in supporting the group, and the ACS officially cosponsored the 1st NOA Conference for "evaluating the molecular mechanism of accelerated and normal wound healing processes", thus ignoring the insurmountable gap which persisted between the vision and the experimental possibilities:
Nearfield Optical Analysis (NOA) via Nearfield Scanning Optical Microscopy (NSOM) existed since 10 years, however, nobody has so far succeeded to image a living cell under physiological conditions with this method. Two particular reasons seemed to oppose any substantial progress: the problem of operations in aqueous environments, and the "low optical contrast", characteristic of optically investigated unlabeled living cells. The first problem has been solved at the European Nearfield Scanning Optical Microscopy (ENSOMA) Laboratory by the use of hydrophobically coated biosensors, and the milestone could be presented during the 1st NOA Conference in November 2000 [4].
NSOM [5] has produced highest optical resolution that has ever been achieved, a method exploiting the energy transfer from the tip of an optical element (tip diameter 20nm) oscillating within the characteristic range of the energy transfer (~ 10nm) in the nearfield of the surface to be analyzed. Irradiation-induced energy transfer between excited molecules (emitter) and receptor molecules (acceptor) positioned in the proximity of the emitter molecules via spacer molecules, has been confirmed experimentally (Kuhn, 1970).
During the 2nd NOA Conference, held in May 2001, and cosponsored by NASA and DARPA: 2nd International NASA/DARPA Photobiology Conference on Nearfield Optical Analysis (NOA), at the National Aeronautics and Space Administration - Johnson Space Flight Center (NASA-JSC), Houston, TX, U.S.A., we went, en route to solve the "low optical contrast" problem, one step further and demonstrated that clear NOA images could be obtained from nanobacteria in an aqueous environment - an encouraging advance [6]. The 2nd NOA - with more than 40 international photobiology peers - promoted both LLLT and NOA, with the special result that LLLT/LILAB could advance in less than six month to scientific acceptance in three fields: civil, military and space relevant.
The scientific breakthrough came just before the 3rd NOA (Brazil, June, 2002) in form of the publication of clear nanoscale images of human dentin in an aqueous environment [7], and the very first images of living endothelial cells in liquid cell culture medium [8], thus opening an optimistic perspective to a direct analysis of LLLT mechanisms. The cells were attached to polished titanium discs and analysed with hydrophobically coated optical biosensors mounted to a conventional NSOM microscope. We are presently in an era where cellular imaging and photobiology is becoming important to wide ranging disciplines. The recent advances in NOA have provided us with the technology necessary for identifying relationships between cellular activities and various photonic stimuli - on Earth and in space. Cellular imaging of living cells via NOA has been recognized as extremely beneficial, in particular for biomedical applications [3] and in tissue bioengineering [9].
Our vision, presumably realizable via NOA, could be generalized as: Time resolved analysis of the LLLT induced molecular mechanisms in living cells, with the light energy densities and intensities conform to the LILAB-equation, and with different wavelengths of coherent and non-coherent light, allowing to systematically understand and optimise the LLLT parameters.
References [1] Sommer, A.P, Pinheiro, A.L.B., Mester, A.R., Franke, R.P., Whelan, H.T. Biostimulatory [2] Al-Watban, F. Comparison between Laser Therapy and Pharmacological Treatments in Accelerating Wound Healing - an extended study in: Proc. 2nd International conference on nearfield optical analysis: photodynamic therapy & photobiology effects. Johnson Space Flight Center, May 2001, Houston, TX, NASA Conference Publication, in press. [3] Preface, Proc. 1st International Workshop on Nearfield Optical Analysis, Reisensburg, Germany, November 2000, (ed. A.P. Sommer) J. Clin. Laser Med. & Surg., 19, 109-112, 2001. [4] Sommer, A.P. Components for NOA of Biosystems and Nanoscale Resolution, in: Proc. 1st International Workshop on Nearfield Optical Analysis, Reisensburg, Germany, November 2000, (ed. A.P. Sommer), J. Clin. Laser Med. & Surg., 19, 112, 2001. [6] Sommer, A.P. Nearfield Optical Analysis (NOA) via Hydrophobic Optical Elements & Low Intensity Light Activated Biostimulation (LILAB) Effect of NOA. Proc. 2nd International conference on near-field optical analysis: photodynamic therapy & photobiology effects. Johnson Space Flight Center, May 2001, Houston, TX, NASA Conference Publication, in press. [7] Sommer, A.P., Franke, R.P. Hydrophobic optical elements for near-field optical analysis (NOA) in liquid environment - a preliminary study. Micron, 33, 227-231, 2002. (Medline) [8] Sommer, A.P., Franke R.P. Near-Field Optical Analysis of Living Cells in Vitro. Journal of Proteome Research, 1, 111-114, 2002. (ACS/ASAP-article) [9] A.P. Sommer, Novel Low Intensity Light Activated Biostimulation Paradigm, in: Abstracts of the Second Congress of the North American Association for Laser Therapy & First Consensus Conference on Laser Medicine, Photobiology and Bioengineering of Tissue Repair, Atlanta, GA, March 2002.
| |
A year ago, Mr Djoko, visited my office due to herpetic neuralgia. Sent by prpfesor Adhi Juanda, dermato-venerologyst,. The vesicles already diminished, but his visual analoge scale (v a s) for pain , above 7. Still some hyperpigmentations (spots) area left chest, intercostals space 3,4 , and 5 betwenn sternum and axilla anterior line.
I try to blok the nerve, . two centimeter to the left from body of 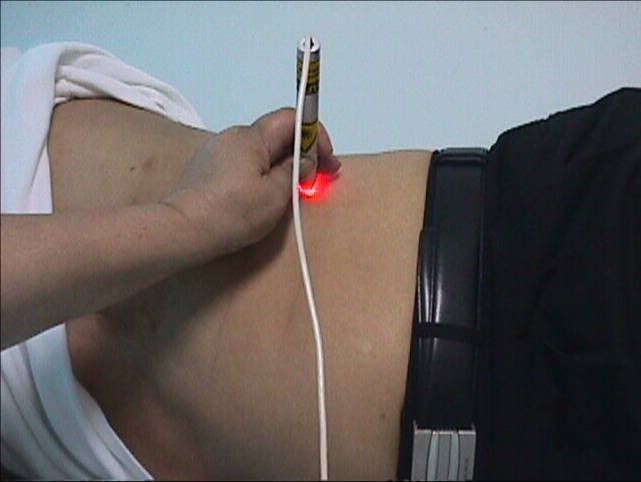 the spine , intercostals 1,2, 3 4 and 5; 5 poiints, 5 Joule per point . same dose at posterior line axillary, and area of spots 3 points, 5 joule every point. The total dose was: 65 Joule. Suddenly after treatment, the vas decreased become 3. (Diode laser 810 nm 50 mW)
the spine , intercostals 1,2, 3 4 and 5; 5 poiints, 5 Joule per point . same dose at posterior line axillary, and area of spots 3 points, 5 joule every point. The total dose was: 65 Joule. Suddenly after treatment, the vas decreased become 3. (Diode laser 810 nm 50 mW)
The pain disappear after 10 treatment (everyday , axept Sunday), but after a week, he felt discomfort again with vas between 3 and 4..
Almost 1 year he come ones a week, with pain vas between 1 - 2.. I give trancutaneus ( half hour), and probe at the points he feel pain, ( 10 minutes). No pain at the end of the the treatment. (Diode 650 nm; transcutaneus 50 mW; probe 50 mW)
 Two months a go, he retired from his office , and begin his own business. He feel more comfort, and the pain no annoying anymore, He still visit my office ones a month, just to make sure no pain again.
Two months a go, he retired from his office , and begin his own business. He feel more comfort, and the pain no annoying anymore, He still visit my office ones a month, just to make sure no pain again.
Discussion:
I used the laser to manage the pain by blocking the nerve. It is not usual for herpetic neuralgia. According to Kert and Rose, they suggest treatment at the vesicle.
Also the dose, rather higher than guidance, they recommend 1 – 2 Joules per point, with total about 15 – 20 Joules.
Is there any connection between the pain and emotional problem ???
Drugs :
Ubi quinon given a long with laser. Ubi quinon works at mitochondria, as well as low laser. Methycobalamin, 500 mg, twice daily. At the first month, drugs for pain also administered.. NSAID, ones a day during first month, after that, he drink, just if the pain going increase more than vas 2.
Here some abstracts :
DOUBLE BLIND CROSSOVER TRIAL OF LOW LEVEL LASER THERAPY (LLLT) IN THE TREATMENT OF POST HERPETIC NEURALGIA
Kevin C Moore MB ChB FRCA Naru Hira. Parswanath Kramer, Copparam Jayakumar & Toshio Ohshiro
Department of Anaesthesia, The
Post herpetic neuralgia can be an extremely painful condition which in many cases proves resistant lo all the accepted forms of treatment. It is frequently most severe in the elderly and may persist for years with no predictable course. This trial was designed as a double blind assessment of the efficacy of low level laser therapy (LLLT) in the relief of the pain of post herpetic neuralgia with patients acting as their own controls. Admission to the trial was limited to patients with established post herpetic neuralgia of at least six months duration and who had shown little or no response to conventional methods of treatment. Measurements of pain intensity and distribution were noted over a period of eight treatments in two groups of patients each of which received four consecutive laser treatments. The results demonstrate a significant reduction in the pain intensity and distribution following a course of low level laser therapy.
Laser Therapy. 1988; 1: 7.
![]()
EFFICACY OF LOW REACTIVE-LEVEL LASER THERAPY (LLLT) FOR PAIN ATTENUATION OF POSTHERPETIC NEURALGIA
Osamu Kemmotsu, Kenichi Sato, Hitoshi Furumido, Koji Harada, Chizuko Takigawa, Sigeo Kaseno, Sho Yokota, Yukari Hanaoka and Takeyasu Yamamura
Department of Anaesthesiology, Hokkaido University School of Medicine, N-15, W-7, Kita-ku,
The efficacy of low reactive-level laser therapy (LLLT) for pain attenuation in patients with postherpetic neuralgia (PHN) was evaluated in 63 patients (25 males, 38 females with an average age of 69 years) managed at our pain clinic over the past 4 years. A double blind assessment of LLLT was also performed in 12 PHN patients. The LLLT system is a gallium aluminium arsenide (GaAlAs) diode laser (830 nm, 60 mW continuous wave) Pain scores (PS) were obtained using a linear analog scale (0 to 10) before and after LLLT. The immediate effect after the initial LLLT was very good (PS: 0-3) in 26, and good (PS: 7-4) in 30 patients. The long-term effect at the end of LLLT (the average number of treatments 36 +/- 12) resulted in no pain (PS: 0) in 12 patients and slight pain (PS: 1-4) in 46 patients. No complications attributable to LLLT occurred. Although a placebo effect was observed, decreases in pain scores and increases of the body surface temperature by LLLT were significantly greater than those that occurred with the placebo treatment. Our results indicate that LLLT is a useful modality for pain attenuation in PHN patients and because LLLT is a non invasive, painless and safe method of therapy, it is well acceptable by patients.
0898-5901/91/020071-05$05.00 Ì 1991 by John Wiley & Sons, Ltd.
 WHAT IS SHINGLES?
WHAT IS SHINGLES? Shingles is a very painful disease caused by the same herpes virus that causes chicken pox (varicella zoster virus). Like other herpes viruses, the varicella-zoster virus has an initial infectious stage, (chicken pox) followed by a dormant stage. Then, with no warning, the virus becomes active again. About 20% of people who have had chickenpox will eventually develop shingles.
This reactivation of the virus is most likely to occur in people with a weakened immune system. This includes people with HIV disease, and anyone over 50 years old.
Herpes zoster lives in nerve tissue. Outbreaks of shingles start with itching, numbness, tingling or severe pain in a belt like pattern on the chest, back, or around the nose and eyes. In rare cases, herpes can infect the facial or eye nerves. This can cause outbreaks around the mouth, on the face, neck, and scalp, in and around the ear, or at the tip of the nose.
Shingles outbreaks are almost always on just one side of the body. Within a few days, a rash appears on the skin area related to the inflamed nerve. Small blisters form and fill with fluid. Later they break open and develop crusty scabs.
If the blisters are scratched, someone with shingles might develop a skin infection. This could require treatment with antibiotics and might cause scars.
In most cases, the rash goes away within a few weeks, but in some cases, severe pain can last for months or even years. This condition is called "post herpetic neuralgia."
Shingles is not one of the infections that leads to a diagnosis of AIDS.
A recent study of people with HIV found the highest rates of shingles in:
Shingles can occur in people with HIV shortly after they start taking strong antiviral medications. These cases of shingles are believed to be a sign of a recovering immune system.
Shingles can only occur after someone has had chickenpox. If someone who has already had chickenpox comes into contact with the fluid from shingles blisters, they will not "catch" shingles. However, people who have not had chickenpox could become infected with herpes zoster and develop chickenpox. They should avoid contact with the shingles rash or with any materials that may have touched the shingles rash or blisters.
Several types of drugs are used to treat shingles. They include anti-herpes drugs, and several types treatments for pain.
Anti-herpes drugs: The standard treatment for shingles is the drug acyclovir, which can be given orally (in pill form) or intravenously in more severe cases.
Recently, two new drugs have been approved for the treatment of shingles: famciclovir and valacyclovir. Both famciclovir and valacyclovir are taken three times each day, compared to five times for acyclovir. All of these drugs work best when they are started within the first three days after the shingles pain begins.
 Nerve blockers: Doctors often prescribe various pain medications for people with shingles. Because the pain of shingles can be so intense, researchers have looked for other ways to block the pain.
Nerve blockers: Doctors often prescribe various pain medications for people with shingles. Because the pain of shingles can be so intense, researchers have looked for other ways to block the pain.
Injections of anesthetic drugs and/or steroids are being studied as nerve blockers. These can be injected either into peripheral nerves, or into the spinal column (central nervous system.)
Skin Treatments: Several creams, gels and sprays are being studied. These provide temporary relief from pain. Capsaicin, the chemical that makes chili peppers hot, has shown good preliminary results. In addition, in 1999 the FDA approved a patch form of the anesthetic lidocaine. The patch, called Lidoderm, provides pain relief for some people with shingles. Because it is applied to the skin, it has less risk of side effects than pain medications taken in pill form. For more information, see the Endo Laboratories web site at http://www.lidoderm.com/
Other Pain Medications: A new drug, pregabalin, was approved in late 2004 but is not yet available. Some drugs normally used to treat depression, epilepsy, or severe pain are sometimes used for the pain of shingles. These can have a variety of side effects. Nortriptyline is the antidepressant most frequently used for shingles pain.
Currently, there is no way to predict an outbreak of shingles, and there is no medication approved to prevent it.
However, researchers have shown that giving older people a stronger form of the chicken pox vaccine used for children can boost the type of immunity believed necessary to hold the virus in check. The researchers hope to show that this increased immunity will result in a lower risk of shingles in later life. Merck is developing a shingles vaccine. In a large clinical trial, it reduced shingles illness by about 60%. However, it was only tested in adults over age 60. People wih weakened immune systems were excluded so its value for people with HIV is unknown.




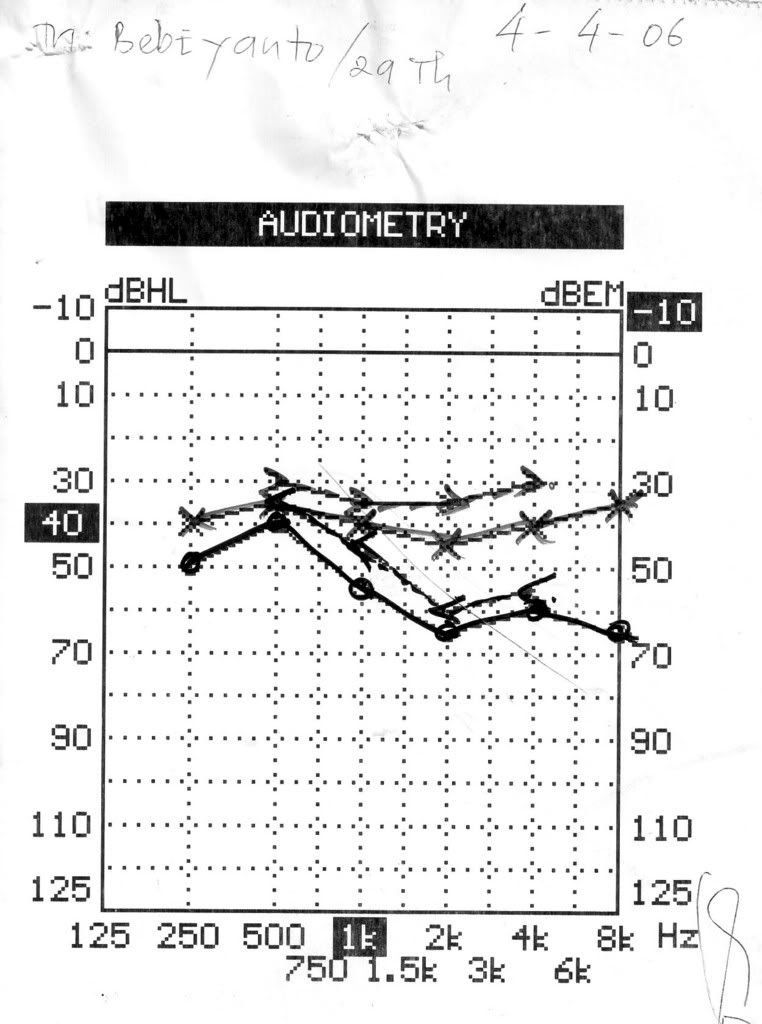
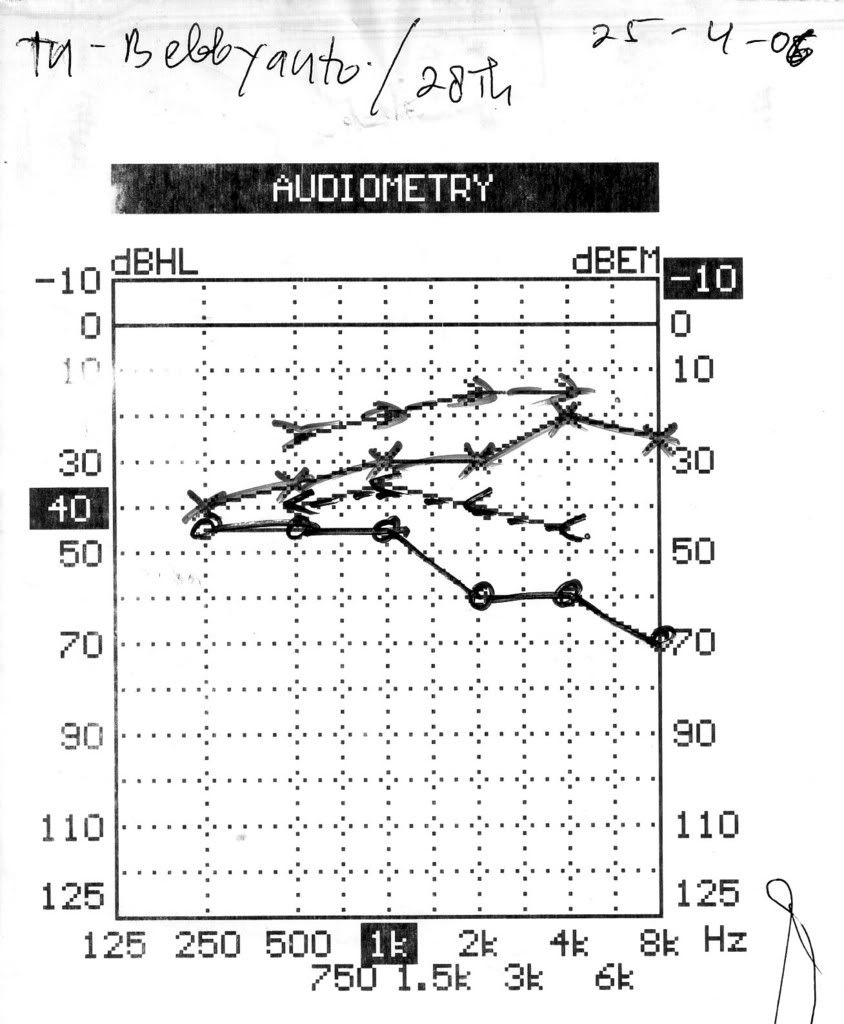
A young man , 29 years old, suffered from hearing impairment
Low level laser administered for 10 times, used:
ILIB (Intravascular Laser Irradiation on Blood) and
Ear probe –pulses
Length of time : 60 minutes
Results:
Using audiometry
Tinitus decrease, cephalgia : no more
 The inner mitochondrial membrane mm is a large collector surface folded onto a small total volume. All nutritive molecules (fats, proteins and glucose) are oxidized within the cell to the last molecular nutritive component, that is, pyruvate. The pyruvate is then imported into the cellular power plant, where it disintegrates into carbon dioxide and water in the immediate proximity of the collector surface of the mitochondrion. The molecular bond energy thus released, which corresponds with visible, ultraviolet and infrared light as far as its wavelength and frequency is concerned, is utilized by the mitochondrion to produce the cellular fuel ATP.
The inner mitochondrial membrane mm is a large collector surface folded onto a small total volume. All nutritive molecules (fats, proteins and glucose) are oxidized within the cell to the last molecular nutritive component, that is, pyruvate. The pyruvate is then imported into the cellular power plant, where it disintegrates into carbon dioxide and water in the immediate proximity of the collector surface of the mitochondrion. The molecular bond energy thus released, which corresponds with visible, ultraviolet and infrared light as far as its wavelength and frequency is concerned, is utilized by the mitochondrion to produce the cellular fuel ATP. The collector surface of our cellular power plant is enlarged by the mushroom-shaped protrusions of the inner mitochondrial membrane mm. The molecular bond energy mb of the pyruvate is released in the form of light energy le.
The collector surface of our cellular power plant is enlarged by the mushroom-shaped protrusions of the inner mitochondrial membrane mm. The molecular bond energy mb of the pyruvate is released in the form of light energy le. Low level laser light lll is compressed light from the red spectrum of the visible part of electro-magnetic radiation (= light). It reaches the cellular power plants of low-lying cells as well and is absorbed by their collector surfaces as an additional source of energy. The cellular power plants can thus produce more ATP. The cellular energy is the fuel the inner ear cells strives after and needs. A sufficiently high supply of cellular energy enables our inner ear cell to work under optimum conditions and is the essential prerequisite to ensure a successful self-healing process.
Low level laser light lll is compressed light from the red spectrum of the visible part of electro-magnetic radiation (= light). It reaches the cellular power plants of low-lying cells as well and is absorbed by their collector surfaces as an additional source of energy. The cellular power plants can thus produce more ATP. The cellular energy is the fuel the inner ear cells strives after and needs. A sufficiently high supply of cellular energy enables our inner ear cell to work under optimum conditions and is the essential prerequisite to ensure a successful self-healing process.















