


 This is picture of his left knee, bigger than his right
This is picture of his left knee, bigger than his right 



Here a copy from LIGHT SPEED
Gout & Laser Therapy
By Fred Kahn, MD, FRCS(C)
President Meditech International Inc.
Gout
Gout (also referred to as gouty arthritis) is a debilitating form of arthritis caused by the accumulation of uric acid crystals in the joints and tendons. It is an intensely painful disease that results from an increased uric acid concentration in the bloodstream. The most frequent location of symptoms is the 1st toe (75% of initial attacks), although it can also affect many other joints such as the ankle, knee, digits and spine.
Gout may be associated with renal disease, diabetes, obesity, leukemia and also the result of the use of diuretics.
Pathogenesis
Acute gout presents without warning. The exact cause of the disease is not known, although it is linked to a deficiency in purine metabolism. It can also be associated with minor trauma, overindulgence in purine-rich food, alcohol, surgery, fatigue, emotional and other stress. Purine is an organic compound that is common in the body and is metabolized into uric acid. Individuals suffering with gout usually have an increased concentration of uric acid in the blood, the result of increased production of uric acid and/or an impaired excretion thereof. This increased concentration of uric acid (hyperuricema) results in local deposits of monosodium urate (MSU) crystals in relatively avascular tissues (i.e. cartilage, tendons, ligaments, etc.) around the cooler distal peripheral joints (Figure 4). In severe long standing cases, this condition can also result in MSU crystals being deposited in larger central joints as well as also the kidneys (renal calculi). Uric acid is normally processed in the kidneys into a form of urate for excretion.
Stages
Gout can be subdivided into four distinct stages:
1. Asymptomatic
2. Acute
3. Intercritical
4. Chronic
In the first stage (asymptomatic), the uric acid levels in the blood increase, but there are no symptoms. The initial attack of gout marks the acute stage. These attacks generally resolve rapidly although severe attacks can last several days and can even extend several weeks.
Low Intensity Laser Therapy has been clinically demonstrated to shorten the duration of the initial outbreak in addition to relieving the pain associated with this stage. Following the initial attack, the patient enters a period of dormancy, known as the intercritical or symptom-free stage that may last for a long period of time. The majority of gout sufferers experience their second attack generally within 6 months to 2 years. In the chronic stage of the disease, attacks of gout become more frequent and polyarticular (affecting more than one joint). Large tophi (deposits of crystals) can be found deposited in many joints during this phase.
Signs and Symptoms
The onset of gout is generally confined to nocturnal pain in a single joint (monoarticular), although it can be associated with multiple joints. The pain becomes progressively more severe and at times can be excruciating. The symptoms often mimic those of acute infection with edema, elevated temperature and erythema. The soft tissues overlying the joint are usually extremely tender and in some instances even the presence of blankets touching the skin can be irritating. The overlying skin is tense, warm, shiny and red or purplish in colour. Fever, tachycardia, chills and malaise may also be present.
The secondary attacks usually affect only one joint and last only a few days, but subsequent attacks can affect several joints simultaneously or sequentially and persist for weeks if left untreated.
Diagnosis
Gout has such a distinct clinical signature that it can often be tentatively diagnosed by history and physical examination alone. Elevated serum urate (7mg/dL) supports the diagnosis but is not specific. This is due to the fact that 30% of the patients have a normal serum urate level at the time of their first attack. The definitive diagnosis of gout can be readily obtained from light microscopy of the joint fluid aspirated from the afflicted area. This will clearly demonstrate intracellular monosodium urate crystals.
Treatment
The first treatment administered should be directed to relieve pain. Conventionally this has consisted of the use of NSAID’s and analgesics to temporarily diminish pain sensation.
Low Intensity Laser Therapy (LILT) properly applied can significantly reduce the pain and swelling associated with acute outbreaks of gout immediately, with concomitant elimination of the requirement for pharmaceuticals. LILT acts rapidly to reduce the inflammation surrounding the joint capsule in addition to relieving the debilitating pain. At our clinics generally there is a total relief of pain following 1 to 3 treatments on sequential days. A recent publication on the use of laser therapy in treating the acute stage of gout demonstrated that “both laser therapy and diclofenac (NSAID) achieved rapid pain relief in patients with acute gouty arthritis, similar in efficacy. Laser therapy was more effective than diclofenac in patients with chronic pyrophosphate arthropathy and in patients with chronic apatite deposition disease”. The article supports that Low Intensity Laser Therapy should be selected as the treatment of choice in acute gout.
Following the reduction of these initial symptoms the conventional therapy is to administer colchicine which reduces the serum concentration of uric acid in the blood. As with most pharmaceuticals, colchicine produces undesirable side effects including GI tract symptoms. Avoiding purine rich foods such as meat, fish, dry beans, mushrooms, alcohol, in addition to consuming purine-neutralizing foods (i.e. fresh fruits and vegetables) could help reduce the concentration of uric acid. Even with a change in diet the success of this approach is limited in reducing the symptoms of gout. In addition to changes in diet, increasing the volume of liquids ingested, particularly water, aids in the body’s ability to excrete uric acid.
Recently Allopurinol has been developed as a long term treatment of gout. This treatment is useful in reducing the serum uric acid levels with concomitant reductions in the outbreaks of gout. Again there are obstacles with this approach as this treatment cannot be administered until after the attack has subsided. Other side effects include GI tract distress, hepatitis and a potentially harmful eczema. An additional negative aspect of this treatment is that it is a lifelong decision; ceasing treatment with Allopurinol causes an almost immediate relapse of gout due to the sudden rise in serum uric acid levels.
Recently, we had 2 complex cases of gout in rapid succession. Routinely, we treat 30-40 cases of gout per annum and in all cases we obtain rapid resolution of symptoms without early recurrence. The majority of patients on initial presentation have been on medications including Indomethacin, Colchicine, Allopurinol, etc. Most patients had continued to have persistent pain and presented in order to obtain more effective alternative therapy. Rapid resolution of pain and inflammation are infallible indicators of change in the affected joints. These two patients noted nearly 100% reduction in pain following their first treatment. Whereas this approach is highly effective, patients should also be cautioned to alter their dietary habits in order to maintain low uric acid levels. Our experience at Meditech indicates that LILT instituted at the onset of pain is the treatment of choice in both acute and chronic gout.

On Wednesday, the rash appeared, He just noticed that his son got varicella about two weeks earlier.
Friday morning, his wife found he was delier. His wife brought him to the hospital. During first hour, the convulsion happened!!
We admitted him to the Intensive Care Unit,
Brain Scan: normal, electrolyte : normal
Consciousness status : somnolent
Convulsion still occur sometimes.
Regiment: medication for viral become the first line.
I have been using ILIB (Intravascular Laser Irradiation on
Blood)
It will be done 10 times, everyday for 10 days
Result:
After 1st administration, the convulsion diminished,
eye contact has become more adequate.
I will write reports on the progress.
The story:
At friday afternoon, I found cyanotic at all of his nails. He bound to the bed, because couldn't lying down quietly. So, I decided to give him ILIB with the dose for brain injured.
The laser (ILIB) began on Saturday morning. opening power for 50 %, administered for 1 hour. In the evening the nurse reported the the convulsion diminished.
Sunday morning , it was eye contact, but not adequatly. The second laser with the same dose. Nurse reported inthe evening, the fever just 38 degree.The followings are some references on chickenpox in adults:
Facts About Chickenpox for Adults
Chickenpox, also known as varicella, is a very contagious disease caused by the varicella-zoster virus. It is spread easily through the air by infected people when they sneeze or cough. The disease also spreads through contact with an infected person's chickenpox blisters. Because chickenpox is very contagious, it is possible for people who have never had chickenpoxnor been vaccinated against it to become infected just by being in a room with someone who has the disease. However, transient exposure is not likely to result in infection.
Symptoms of chickenpox
Early symptoms may include body aches, fever, fatigue, irritability and sore throat. A rash then appears and develops into as many as 250-500 itchy blisters over the entire body, that usually last for 5-7 days and heal with scabs. The rash may even spread into the mouth or other internal parts of the body. The illness is usually not severe, but the risk of hospitalization and
death is increased among adolescents and adults.
Symptoms appear between 10 and 21 days after exposure to the varicellazoster
virus. Persons who were vaccinated against chickenpox may sometimes develop chickenpox disease but the presentation is usually mild, with approximately 50 or fewer red bumps that rarely evolve to blisters.

Low Level Laser Therapy In The Management Of Chronic Myofascial Pain In The Neck
A Gur, AJ Sarac, R Cevik, O Altindag, and S Sarac
Lasers Surg Med, January 1, 2004; 35(3): 229.
Physical Medicine and Rehabilitation, School of Medicine, Dicle University, Diyarbakir, Turkey.
BACKGROUND AND OBJECTIVES: A prospective, double-blind, randomized, and controlled trial was conducted in patients with chronic myofascial pain syndrome (MPS) in the neck to evaluate the effects of infrared low level 904 nm Gallium-Arsenide (Ga-As) laser therapy (LLLT) on clinical and quality of life (QoL).
STUDY DESIGN/PATIENTS AND METHODS: The study group consisted of 60 MPS patients. Patients were randomly assigned to two treatment groups: Group I (actual laser; 30 patients) and Group II (placebo laser; 30 patients). LLLT continued daily for 2 weeks except weekends. Follow-up measures were evaluated at baseline, 2, 3, and 12 weeks. All patients were evaluated with respect to pain at rest, pain at movement, number of trigger points (TP), the Neck Pain and Disability Visual Analog Scale (NPAD), Beck depression Inventory (BDI), and the Nottingham Health Profile (NHP). RESULTS: In active laser group, statistically significant improvements were detected in all outcome measures compared with baseline (P <>
CONCLUSION: This study revealed that short-period application of LLLT is effective in pain relief and in the improvement of functional ability and QoL in patients with MPS. Lasers Surg. Med. 35:229-235, 2004.
Copyright 2004 Wiley-Liss, Inc.

Low-Intensity Laser Irradiation Stimulates Bone Nodule Formation Via Insulin-Like Growth Factor-I Expression in Rat Calvarial Cells
Noriyoshi Shimizu, Kotoe Mayahara, Takeshi Kiyosaki,
Akikuni Yamaguchi, Yasuhiro Ozawa, Yoshimitsu Abiko
Background and Objective: We previously reported that low-intensity laser irradiation stimulated bone nodule formation through enhanced cellular proliferation and differentiation. However, the mechanisms of irradiation are unclear. Thus, we attempted to determine the responsibility of insulin-like growth factor (IGF)-I for the action observed.
Study Design/Materials and Methods: Osteoblast-like cells were isolated from fetal rat calvariae and cultured with rat recombinant (r) IGF-I, IGF-I antibody (Ab), and/or the cells were irradiated once (3.75 J/cm2) with a low-intensity Ga-Al-As laser (830 nm). The number and area of bone nodules formed in the culture were analyzed, and IGF-I expression was also examined.
Results: Treatment with rIGF-I significantly stimulated the number and area of bone nodules. This stimulatory effect was quite similar to those by laser irradiation, and this stimulation was abrogated dose-dependently by treatment with IGF-I-Ab. Moreover, laser irradiation significantly increased IGF-I protein and gene expression.
Conclusion: The stimulatory effect of bone nodule formation by low-intensity laser irradiation will be at least partly mediated by IGF-I expression. Lasers Surg. Med. 39:551-559, 2007. © 2007 Wiley-Liss, Inc.
Key words: low-intensity laserl bone formation; IGF-I; bone nodule; calvarial cell; osteoblast




 I asked her to enhance her lung capacity, using incentive spirometry.
I asked her to enhance her lung capacity, using incentive spirometry.
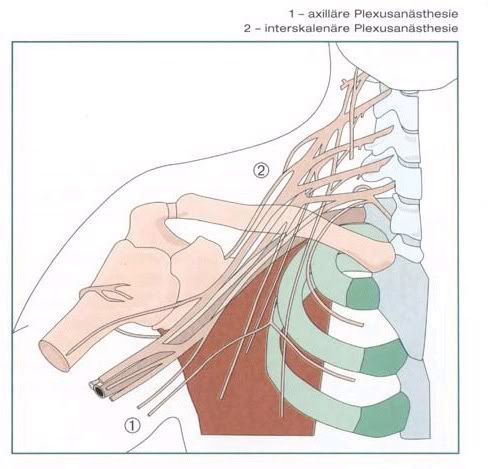
When he came on May 8, 2007, I found deficit sensory 40 % - 60 %. Yes, injury at shoulder site, also could damage the brachial plexus. EMG taken before explained the deficit .
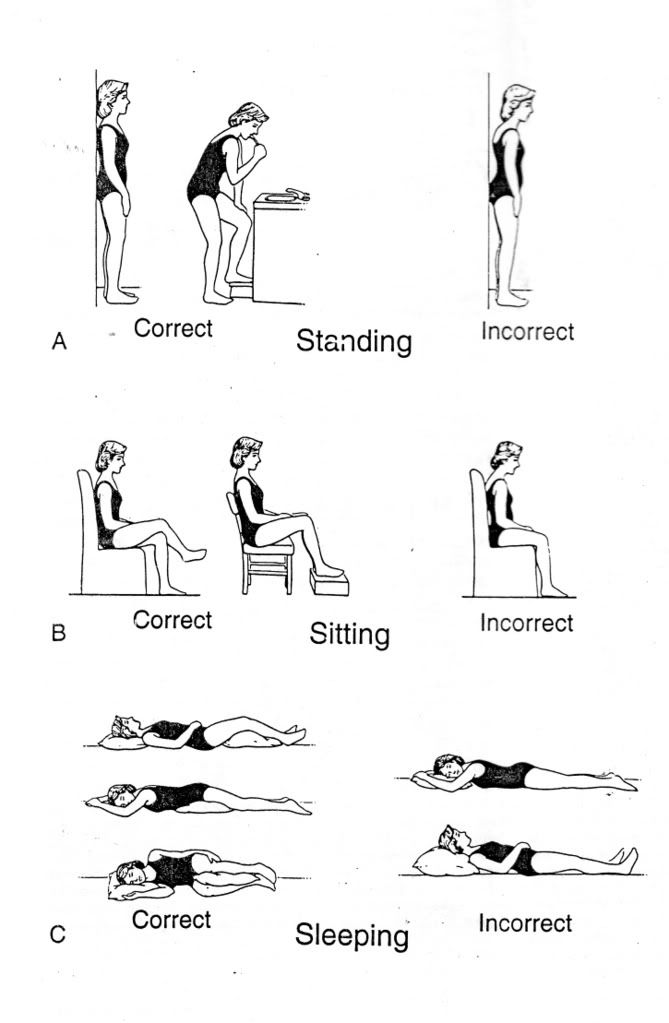
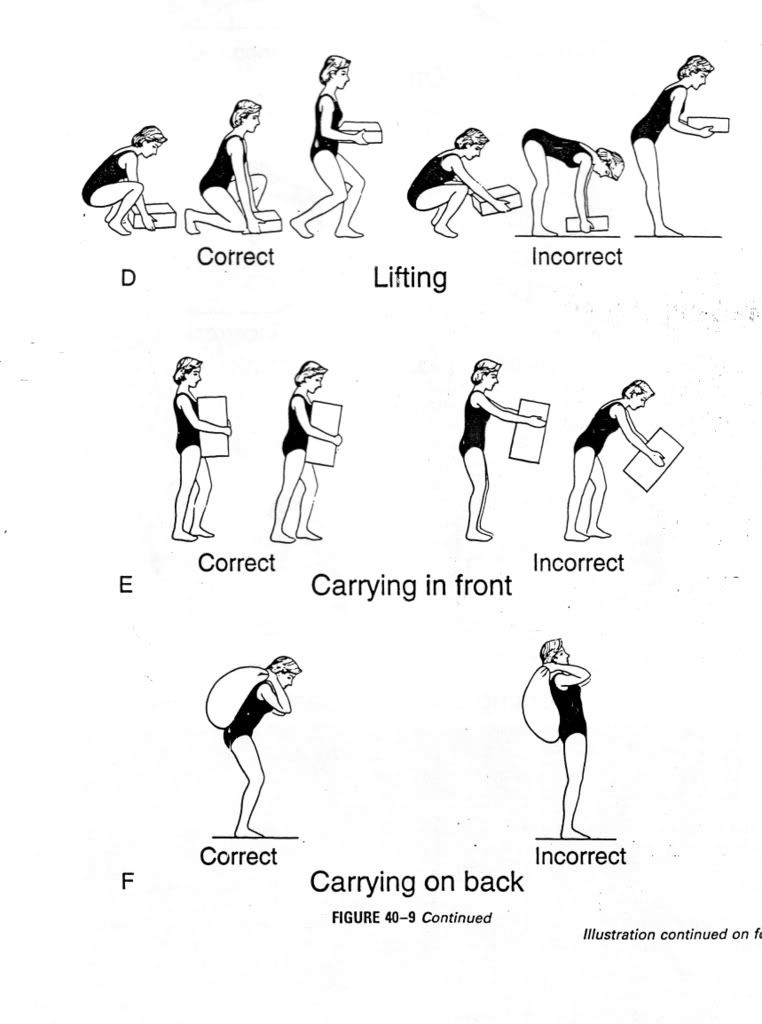
Hospitalized a week, given medicine for pain, drink by the clock; infra red radiation and electrical stimulation; exercise for correction his posture , and prevent further athropy.
Discharge from hospital with toradol 4 times daily, correct posture. Could used right for activity daily living. I asked him to use arm sling and shoulder sling simultaneously. Three times a day exercise to prevent atrophy, take the pain killer by the clock.
Although it is a good case for low laser, it was not suitable for him. He must back to work again , in the middle of the forest. , as soon as possible. If he stay at home, or stay in
As a doctor, especially a physical medicine and rehabilitation specialist ,we must take that as a consider. A team must build, with other doctor , therapist and social worker as needed.
Any comment ?

What is that?
Symptoms
The common symptoms for this kind problem are muscle weakness and cramping, and paralysis like yours, also paresthesias, palpitations, constipation, nausea or vomiting, abdominal cramping, polyuria, nocturia, or polydipsia.1
What is kalium?
Kalium or Potassium is one of the body's major ions. Nearly 98% of the body's potassium is intracellular. The ratio of intracellular to extracellular potassium is important in determining the cellular membrane potential. Small changes in the extracellular potassium level can have profound effects on the function of the cardiovascular and neuromuscular systems.1
Pretty Yulia, Potassium is about working of a cell.
How about the normal level
The reference range for serum potassium level is 3.5-5 mEq/L, with total body potassium stores of approximately 50 mEq/kg (ie, approximately 3500 mEq in a 70-kg person).
Hypokalemia is defined as a potassium level less than 3.5 mEq/L. 1
Moderate hypokalemia is a serum level of 2.5-3 mEq/L. 1
Severe hypokalemia is defined as a level less than 2.5 mEq/L.1
Pathophysiology:
Hypokalemia may result from conditions as varied as renal or GI losses, inadequate diet, transcellular shift (movement of potassium from serum into cells), and medications.
Laser for Hypokalemi
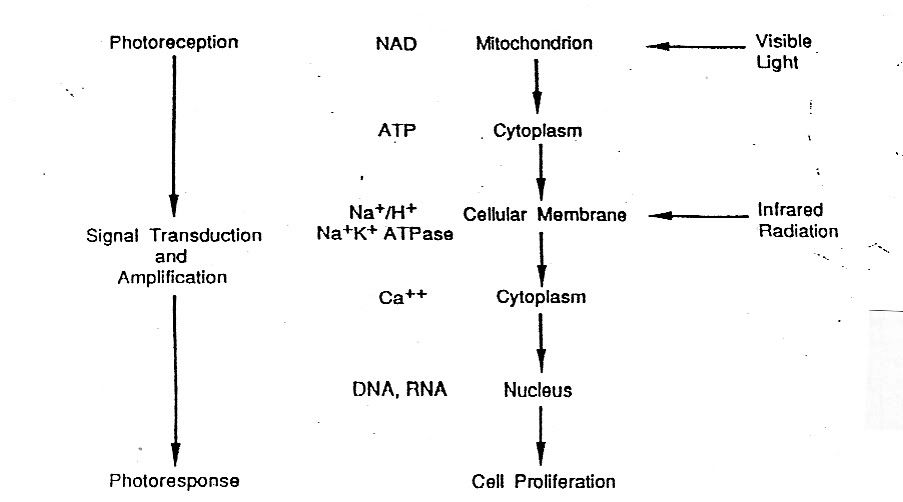
Your father came to me , wonder if Low Level laser Therapy (LLLT) could work on this condition. I found Karu’s model. Karu’s model shows , light is absorbed by components of repiratory chain ( i.e. flavine dehydrogenase, cytochomes and cytochromes oxidase) which causean activation of the respiratory and the oxidation of the NAD pool , which leads to changes in the redox status of oth mitochondria and the cytoplasm. This in turn has an effect on membrane permeability/ transport , with changes in the Na + /H+ ratio and increase Na+/K+ ATPase activity.
How about your's dear?
Inadequate diet and GI problem could explained Yulia's . His father told me, her appetite not so good. She also prone for diarrhea.
So dear, yet LLLT help you , please take times to visit gastroenterologist.
Author: David Garth, MD, Consulting Staff, Department of Emergency Medicine, Mary Washington Hospital : eMedicine Specialties > Emergency Medicine > Endocrine And Metabolic ; Hypokalemia; Last Updated: September 20, 2005




 Five Little Chickens
Five Little Chickens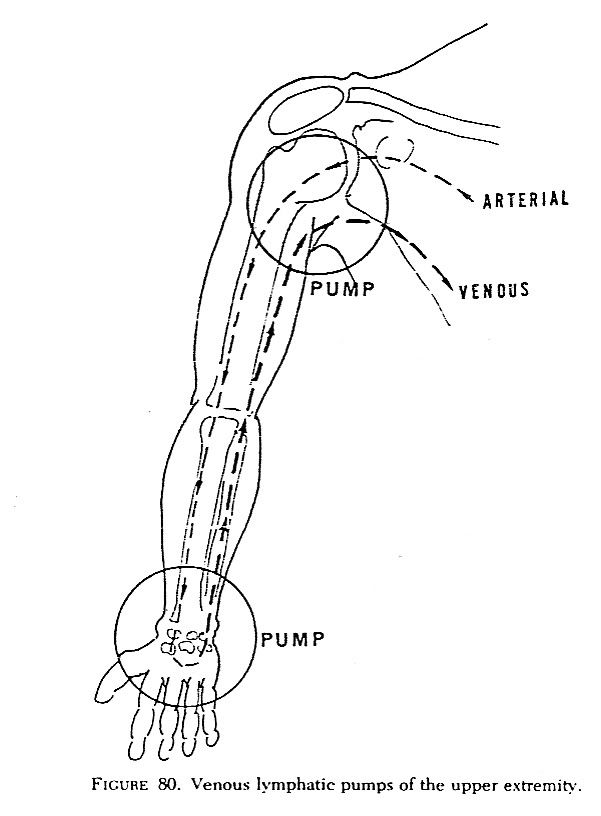
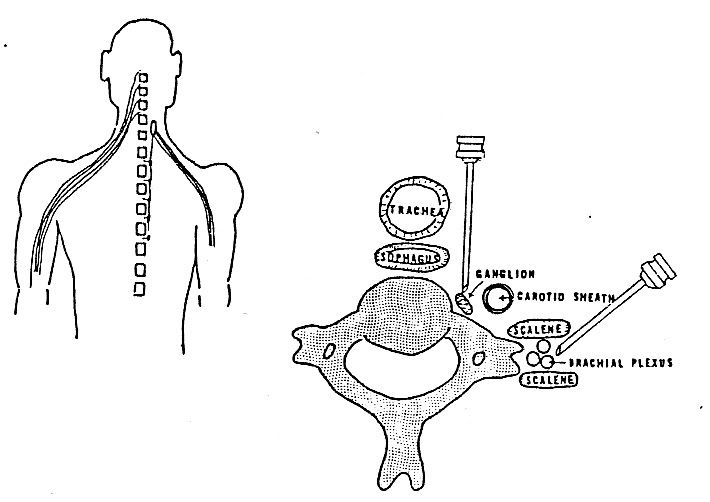
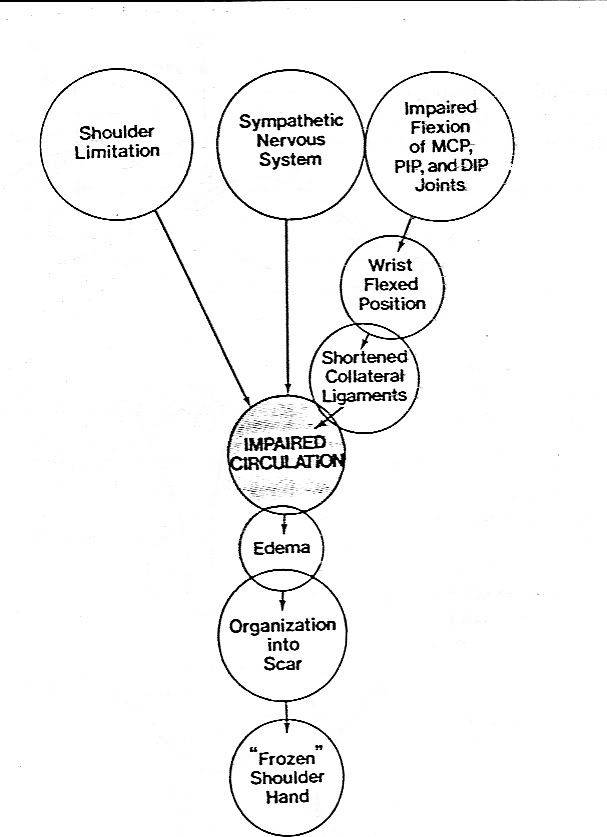
The circulation of upper extremity can be roughly divided into arterial and venous component : first, the arterial component. It is refers to cardiac pumping, proceeding to the distal portion of the extremity. The 2nd are the venous return and lymphatic system. The muscles of the hand and arm force the fluid proximally by means of “pumps”
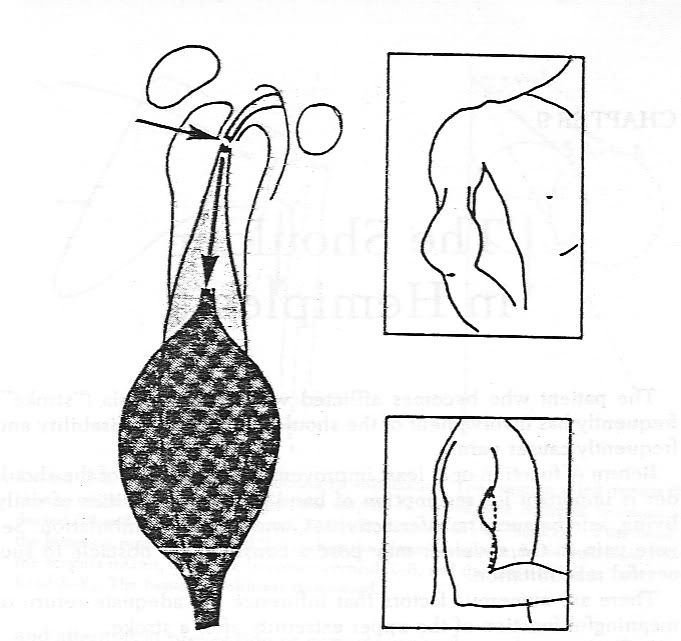
Mr Djoko, got stroke , nearly two years ago, hemiparetic with spasm at his right hand. This was the iniciating factor for his problem. He sent by neurologist due to pain on his right side. I found shoulder limitation , and swollen.

 Mrs Hizkiah, a beautiful nurse, funny, always smile.
Mrs Hizkiah, a beautiful nurse, funny, always smile. She fells pain, aggravated by movement on the wrist and thumb. Dear Hiskiah, it is call De Quervein’s Diseases. Characteristic symptoms can be reproduced by flexing the thumb and  cupping it under the fingers, than flexing the wrist in an ulnar direction which streches the thumb tendons. Lovely Hizkiah, that is the reasoning, why your pain exaggerated after your therapist asked you to made a fist, forcing flex the thumb.
cupping it under the fingers, than flexing the wrist in an ulnar direction which streches the thumb tendons. Lovely Hizkiah, that is the reasoning, why your pain exaggerated after your therapist asked you to made a fist, forcing flex the thumb.
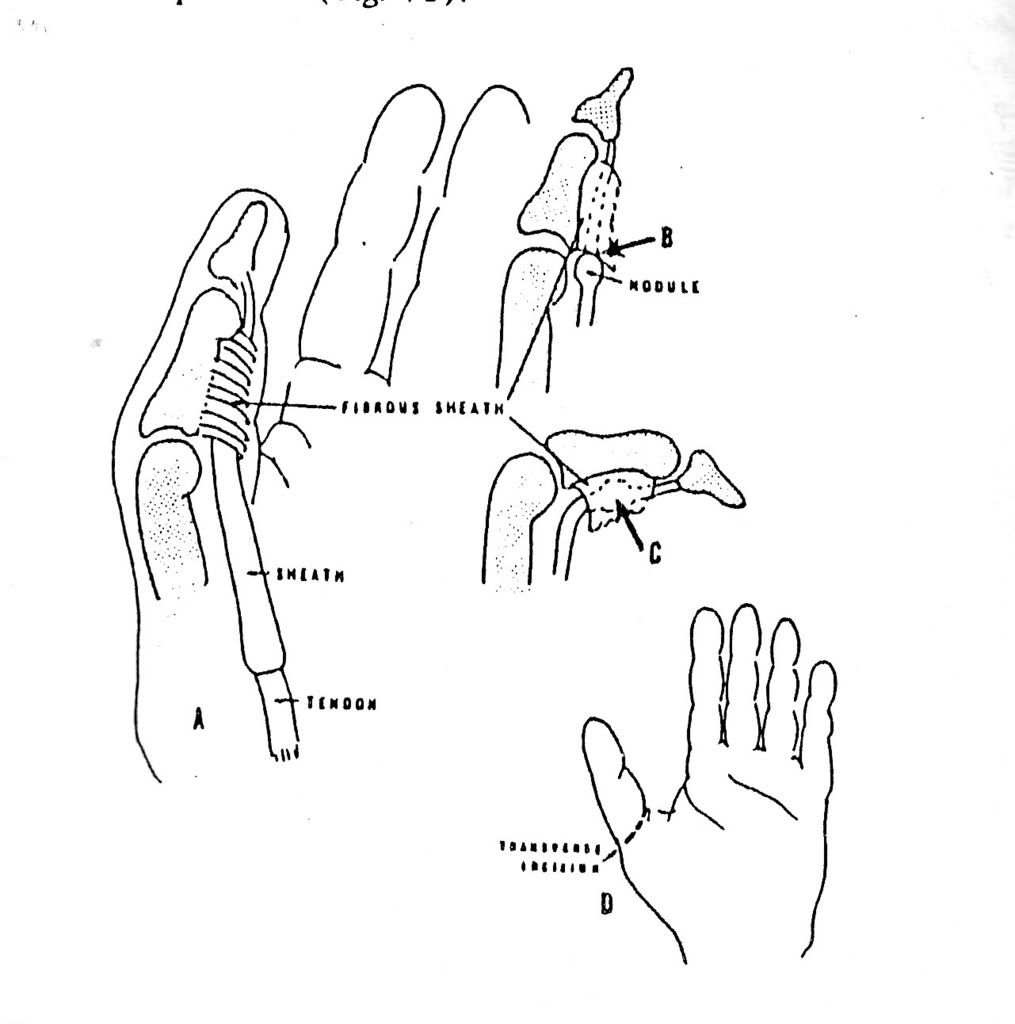
Pity Hizkiah, you also has another problem ., trigger thumb. In this condition your thumb snaps as it flexes and may become locked in flexion or in extension. He didn’t want to harm you, just didn’t knoe that you have another problem.
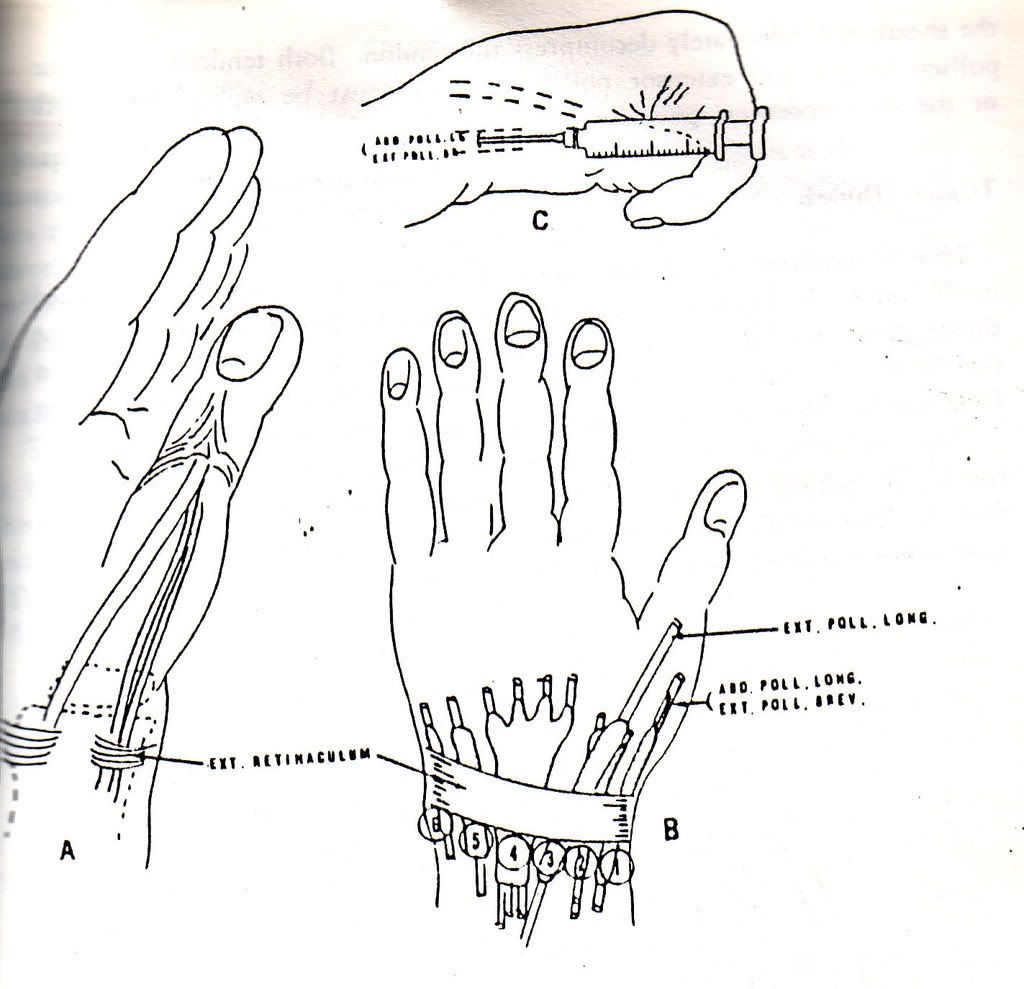
The patology De Quervein’s Diseases is an increased vascularity of the outer sheath that, coupled with edema, thickens the sheath and constricts the enclosed tendon. Treatment requires immobilization with injections of cortisone into the sheath.
My regiment for you is low level laser. Please, no heat modality, due to edema. Low level laser will not increase the temperature above body temperature. It is to reduce the pain and the edema. I am going to immobilize your thumb. But if during four weeks of treatment, there is no relief , may be our surgeon will help you.
The trigger thumb, occurs from thickening of the sheath or the tendon or both which prevents gliding of the tendon within the sheath . Local injections of cortisone into the sheath may result in good recovery . if locking persists , excision of the thickened is performed. That is not my competent. I told you, my first concern is your pain due to De Quervein’s. I use low level laser AMM50, about 830 nm, probe 50 mW, The dose 30 Youles. It is big enough. I am going to decreases the dose if your pain and edema decrease.
(Hand pain and impairment, Rene Cailliet)
De Quervein's
Trigger Thumb




















{kind=link}
{kind=link}
{kind=link}
{kind=link}