
From my office:
My other hearing impairment case:
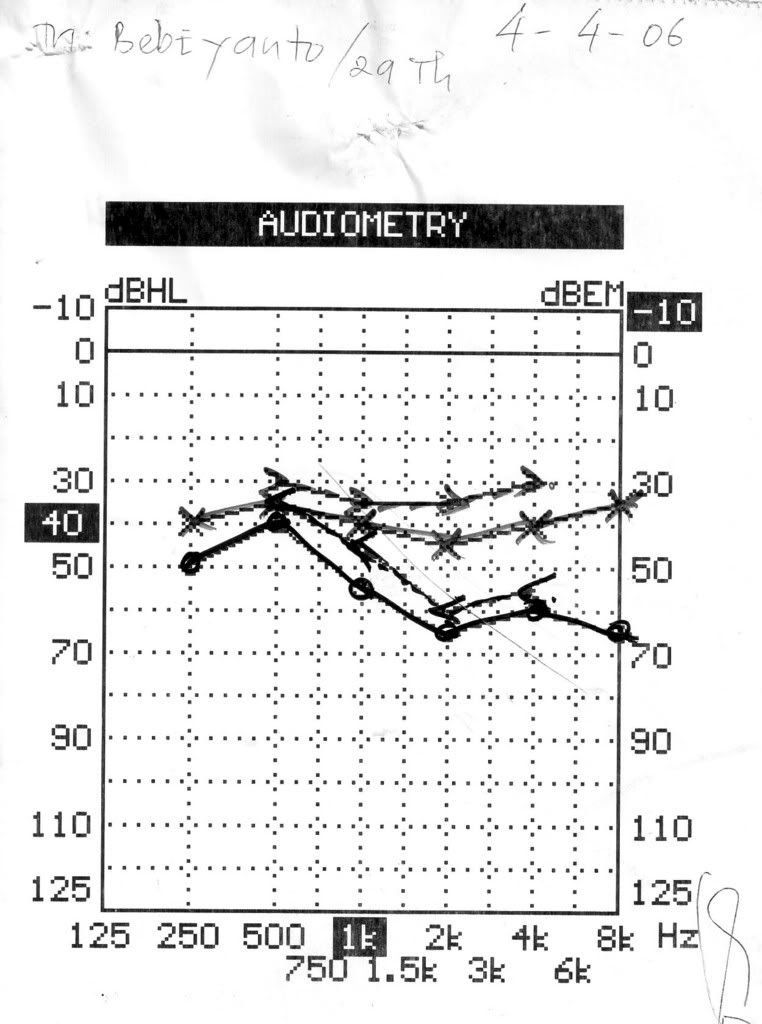
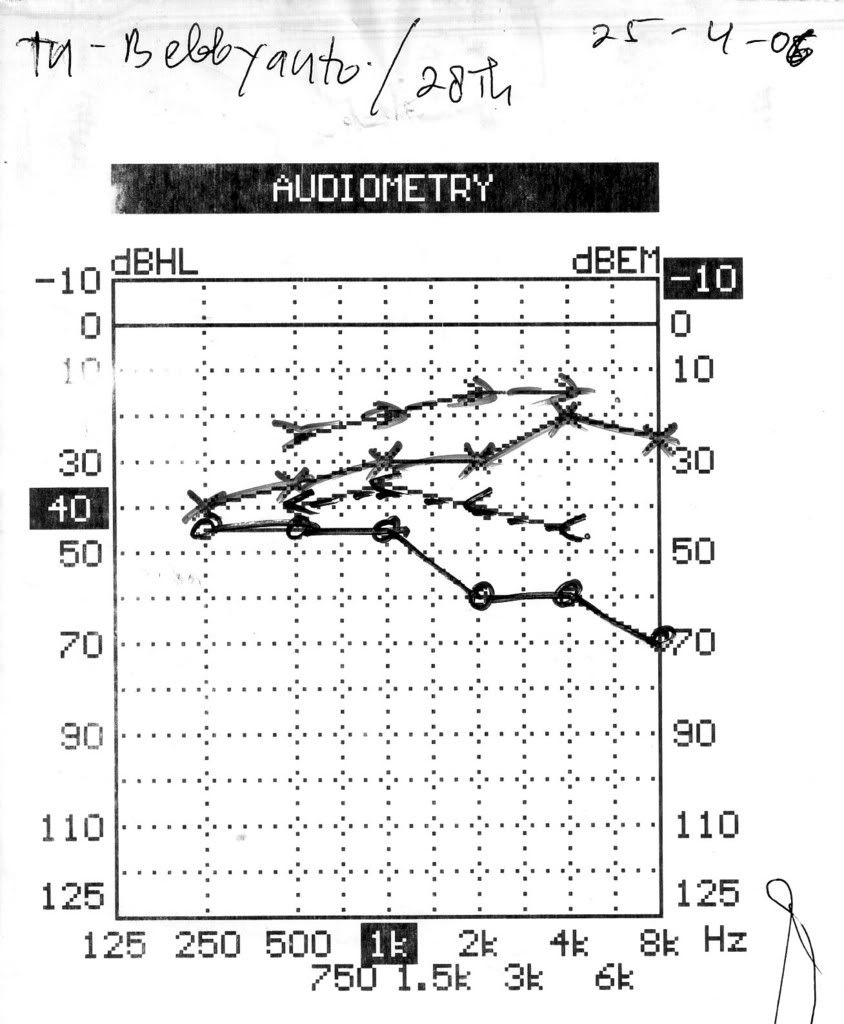
A young man , 29 years old, suffered from hearing impairment
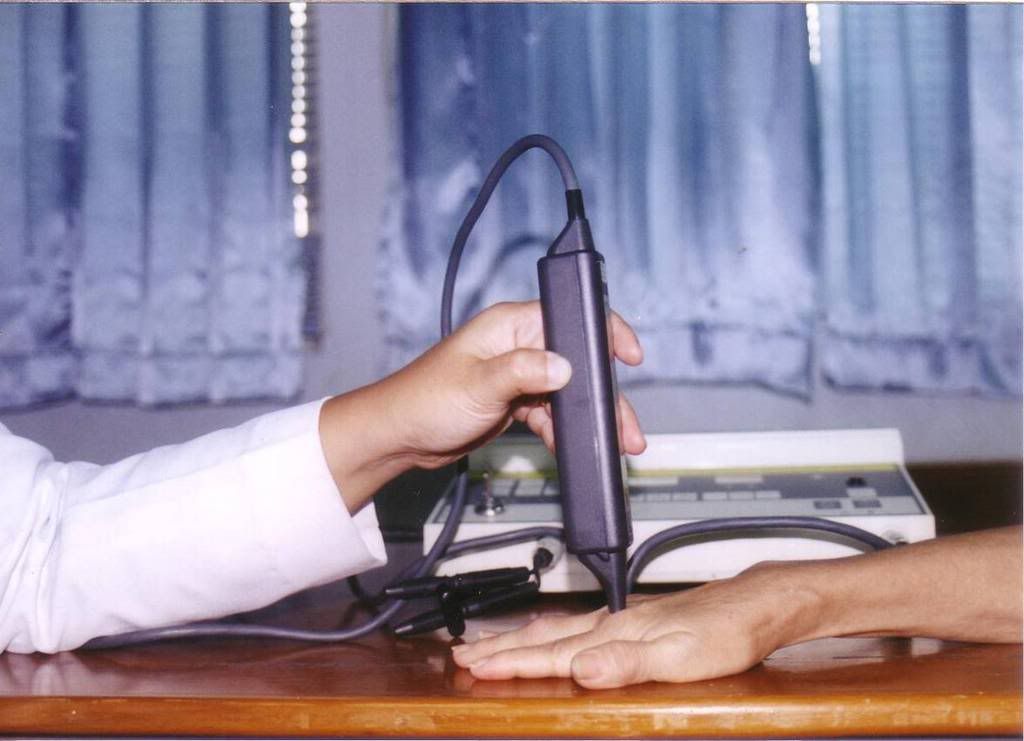
Low level laser administered for 10 times, used:
ILIB (Intravascular Laser Irradiation on Blood) and
Ear probe –pulses
Length of time : 60 minutes
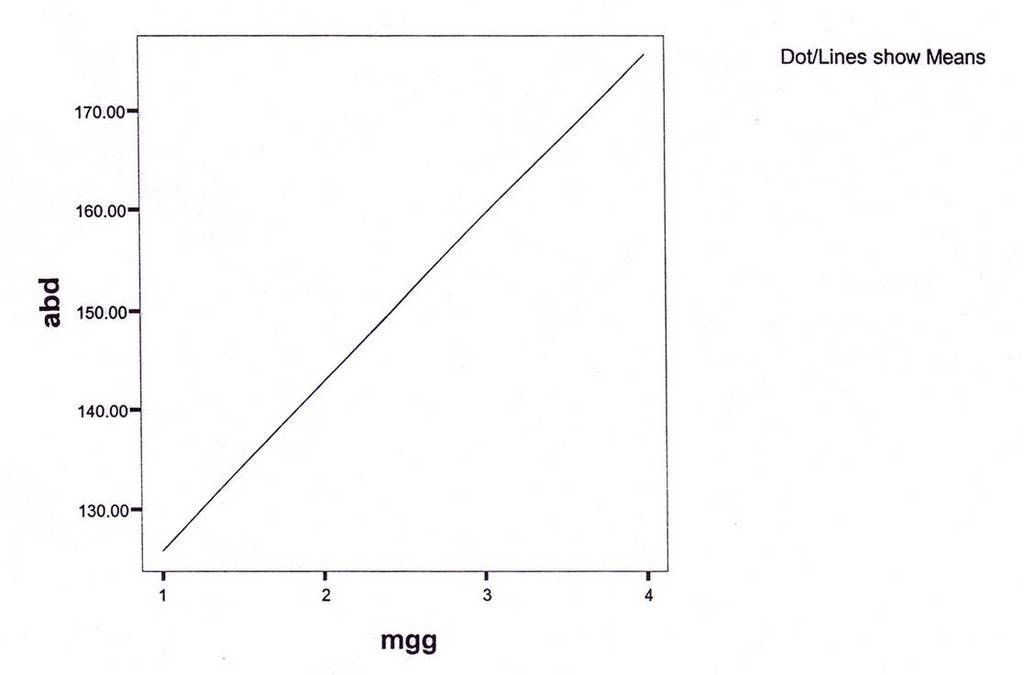
Results:
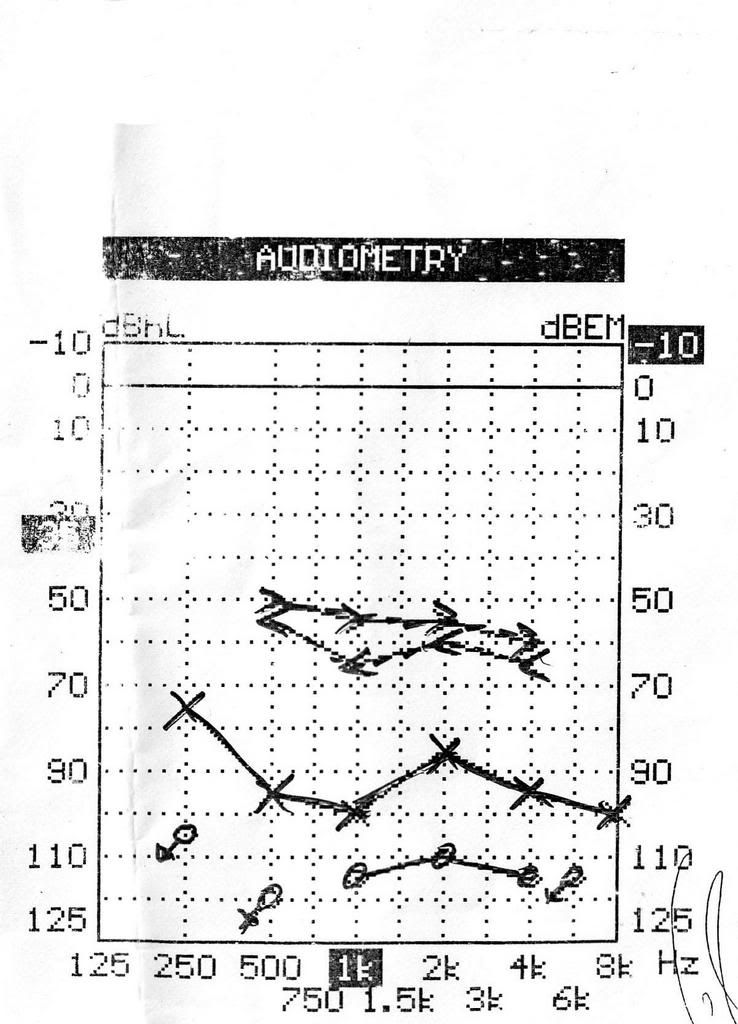
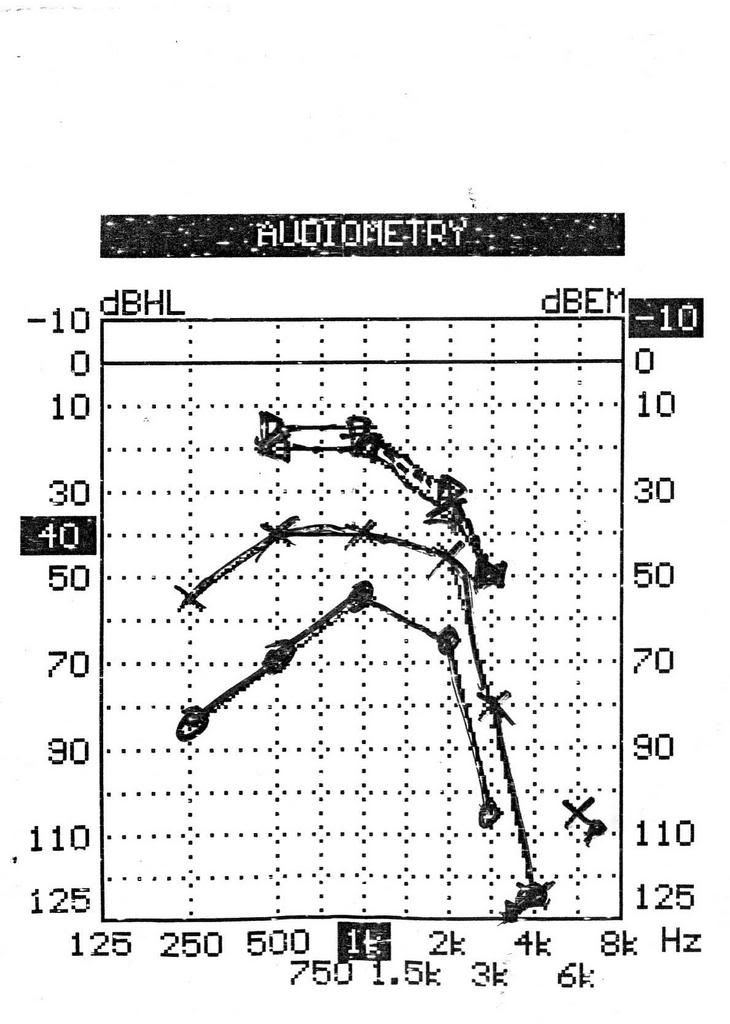
Using audiometry
Tinitus decrease, cephalgia : no more
Discussion :
This young man had no balance problem. he could came by himself to my clinic, so the program : every day for 10 times.
LLLT works for hearing problem, although with tinnitus.
Is everyday and once a week have the same result?
I need more experiences, and I will share with you.
But the key : high dose
This young man had no balance problem. he could came by himself to my clinic, so the program : every day for 10 times.
LLLT works for hearing problem, although with tinnitus.
Is everyday and once a week have the same result?
I need more experiences, and I will share with you.
But the key : high dose
Inner ear diseases & the inner ear
(Dr.med. Lutz Wilden) The inner mitochondrial membrane mm is a large collector surface folded onto a small total volume. All nutritive molecules (fats, proteins and glucose) are oxidized within the cell to the last molecular nutritive component, that is, pyruvate. The pyruvate is then imported into the cellular power plant, where it disintegrates into carbon dioxide and water in the immediate proximity of the collector surface of the mitochondrion. The molecular bond energy thus released, which corresponds with visible, ultraviolet and infrared light as far as its wavelength and frequency is concerned, is utilized by the mitochondrion to produce the cellular fuel ATP.
The inner mitochondrial membrane mm is a large collector surface folded onto a small total volume. All nutritive molecules (fats, proteins and glucose) are oxidized within the cell to the last molecular nutritive component, that is, pyruvate. The pyruvate is then imported into the cellular power plant, where it disintegrates into carbon dioxide and water in the immediate proximity of the collector surface of the mitochondrion. The molecular bond energy thus released, which corresponds with visible, ultraviolet and infrared light as far as its wavelength and frequency is concerned, is utilized by the mitochondrion to produce the cellular fuel ATP. The collector surface of our cellular power plant is enlarged by the mushroom-shaped protrusions of the inner mitochondrial membrane mm. The molecular bond energy mb of the pyruvate is released in the form of light energy le.
The collector surface of our cellular power plant is enlarged by the mushroom-shaped protrusions of the inner mitochondrial membrane mm. The molecular bond energy mb of the pyruvate is released in the form of light energy le.The antennae pigments are capable of absorbing this light energy le and transmit it to our cellular power plant, which can now produce the cellular fuel ATP. The natural solar radiation also stimulates the antennae pigments of the mitochondrion to produce ATP.
 Low level laser light lll is compressed light from the red spectrum of the visible part of electro-magnetic radiation (= light). It reaches the cellular power plants of low-lying cells as well and is absorbed by their collector surfaces as an additional source of energy. The cellular power plants can thus produce more ATP. The cellular energy is the fuel the inner ear cells strives after and needs. A sufficiently high supply of cellular energy enables our inner ear cell to work under optimum conditions and is the essential prerequisite to ensure a successful self-healing process.
Low level laser light lll is compressed light from the red spectrum of the visible part of electro-magnetic radiation (= light). It reaches the cellular power plants of low-lying cells as well and is absorbed by their collector surfaces as an additional source of energy. The cellular power plants can thus produce more ATP. The cellular energy is the fuel the inner ear cells strives after and needs. A sufficiently high supply of cellular energy enables our inner ear cell to work under optimum conditions and is the essential prerequisite to ensure a successful self-healing process.



















{kind=link}