| Wound healing via laser light goes back to Prof. Endre Mester. First reports on his pioneering work started in 1967. For biostimulation he used the coherent light of powerful 50mW He/Ne-lasers (632.8nm). The Mester group has been continuously successful from the beginning. But only a minority of researchers could reproduce the success of the biostimulation experiments. 33 years after introducing the paradigm of photobiostimulation, the LILAB-equation has been anchored into LLLT [1] - establishing the biological limits of the dose (energy density) and the light intensity. Recent laboratory experiments, demonstrating that various individually administered wavelengths of laser light applied at energy densities of the same order induced comparable biological effects in rats, could be interpreted as additional evidence in support of the LILAB-equation [2]. 
During the 1st NOA Conference [3] a multidisciplinary group of ten scientists from Brazil, Denmark, Finland, France, Germany, Hungary, Israel, Saudi Arabia and U.S.A. evaluated possibilities of validating LLLT. One of the discussed visions has been to directly investigate the molecular mechanisms of light-induced wound healing processes occurring in LLLT via Nearfield Optical Analysis (NOA). The vision has been so promising that Attila Pavláth - President ACS - became eventually interested in supporting the group, and the ACS officially cosponsored the 1st NOA Conference for "evaluating the molecular mechanism of accelerated and normal wound healing processes", thus ignoring the insurmountable gap which persisted between the vision and the experimental possibilities:

Nearfield Optical Analysis (NOA) via Nearfield Scanning Optical Microscopy (NSOM) existed since 10 years, however, nobody has so far succeeded to image a living cell under physiological conditions with this method. Two particular reasons seemed to oppose any substantial progress: the problem of operations in aqueous environments, and the "low optical contrast", characteristic of optically investigated unlabeled living cells. The first problem has been solved at the European Nearfield Scanning Optical Microscopy (ENSOMA) Laboratory by the use of hydrophobically coated biosensors, and the milestone could be presented during the 1st NOA Conference in November 2000 [4]. 
NSOM [5] has produced highest optical resolution that has ever been achieved, a method exploiting the energy transfer from the tip of an optical element (tip diameter 20nm) oscillating within the characteristic range of the energy transfer (~ 10nm) in the nearfield of the surface to be analyzed. Irradiation-induced energy transfer between excited molecules (emitter) and receptor molecules (acceptor) positioned in the proximity of the emitter molecules via spacer molecules, has been confirmed experimentally (Kuhn, 1970). 
During the 2nd NOA Conference, held in May 2001, and cosponsored by NASA and DARPA: 2nd International NASA/DARPA Photobiology Conference on Nearfield Optical Analysis (NOA), at the National Aeronautics and Space Administration - Johnson Space Flight Center (NASA-JSC), Houston, TX, U.S.A., we went, en route to solve the "low optical contrast" problem, one step further and demonstrated that clear NOA images could be obtained from nanobacteria in an aqueous environment - an encouraging advance [6]. The 2nd NOA - with more than 40 international photobiology peers - promoted both LLLT and NOA, with the special result that LLLT/LILAB could advance in less than six month to scientific acceptance in three fields: civil, military and space relevant. 
The scientific breakthrough came just before the 3rd NOA (Brazil, June, 2002) in form of the publication of clear nanoscale images of human dentin in an aqueous environment [7], and the very first images of living endothelial cells in liquid cell culture medium [8], thus opening an optimistic perspective to a direct analysis of LLLT mechanisms. The cells were attached to polished titanium discs and analysed with hydrophobically coated optical biosensors mounted to a conventional NSOM microscope. We are presently in an era where cellular imaging and photobiology is becoming important to wide ranging disciplines. The recent advances in NOA have provided us with the technology necessary for identifying relationships between cellular activities and various photonic stimuli - on Earth and in space. Cellular imaging of living cells via NOA has been recognized as extremely beneficial, in particular for biomedical applications [3] and in tissue bioengineering [9].

Our vision, presumably realizable via NOA, could be generalized as: Time resolved analysis of the LLLT induced molecular mechanisms in living cells, with the light energy densities and intensities conform to the LILAB-equation, and with different wavelengths of coherent and non-coherent light, allowing to systematically understand and optimise the LLLT parameters. 
References [1] Sommer, A.P, Pinheiro, A.L.B., Mester, A.R., Franke, R.P., Whelan, H.T. Biostimulatory
Windows in Low Intensity Laser Activation: Lasers, Scanners and NASA's Light Emitting Diode Array System. J. Clin. Laser Med. & Surg., 19, 29-33, 2001. (Medline) [2] Al-Watban, F. Comparison between Laser Therapy and Pharmacological Treatments in Accelerating Wound Healing - an extended study in: Proc. 2nd International conference on nearfield optical analysis: photodynamic therapy & photobiology effects. Johnson Space Flight Center, May 2001, Houston, TX, NASA Conference Publication, in press. [3] Preface, Proc. 1st International Workshop on Nearfield Optical Analysis, Reisensburg, Germany, November 2000, (ed. A.P. Sommer) J. Clin. Laser Med. & Surg., 19, 109-112, 2001. [4] Sommer, A.P. Components for NOA of Biosystems and Nanoscale Resolution, in: Proc. 1st International Workshop on Nearfield Optical Analysis, Reisensburg, Germany, November 2000, (ed. A.P. Sommer), J. Clin. Laser Med. & Surg., 19, 112, 2001.
[5] For a schematic of NSOM and a short principle explanation see: http://www.ensoma.net (click on the Greek letters and in the middle). [6] Sommer, A.P. Nearfield Optical Analysis (NOA) via Hydrophobic Optical Elements & Low Intensity Light Activated Biostimulation (LILAB) Effect of NOA. Proc. 2nd International conference on near-field optical analysis: photodynamic therapy & photobiology effects. Johnson Space Flight Center, May 2001, Houston, TX, NASA Conference Publication, in press. [7] Sommer, A.P., Franke, R.P. Hydrophobic optical elements for near-field optical analysis (NOA) in liquid environment - a preliminary study. Micron, 33, 227-231, 2002. (Medline) [8] Sommer, A.P., Franke R.P. Near-Field Optical Analysis of Living Cells in Vitro. Journal of Proteome Research, 1, 111-114, 2002. (ACS/ASAP-article) [9] A.P. Sommer, Novel Low Intensity Light Activated Biostimulation Paradigm, in: Abstracts of the Second Congress of the North American Association for Laser Therapy & First Consensus Conference on Laser Medicine, Photobiology and Bioengineering of Tissue Repair, Atlanta, GA, March 2002.

|
 Mrs Hizkiah, a beautiful nurse, funny, always smile.
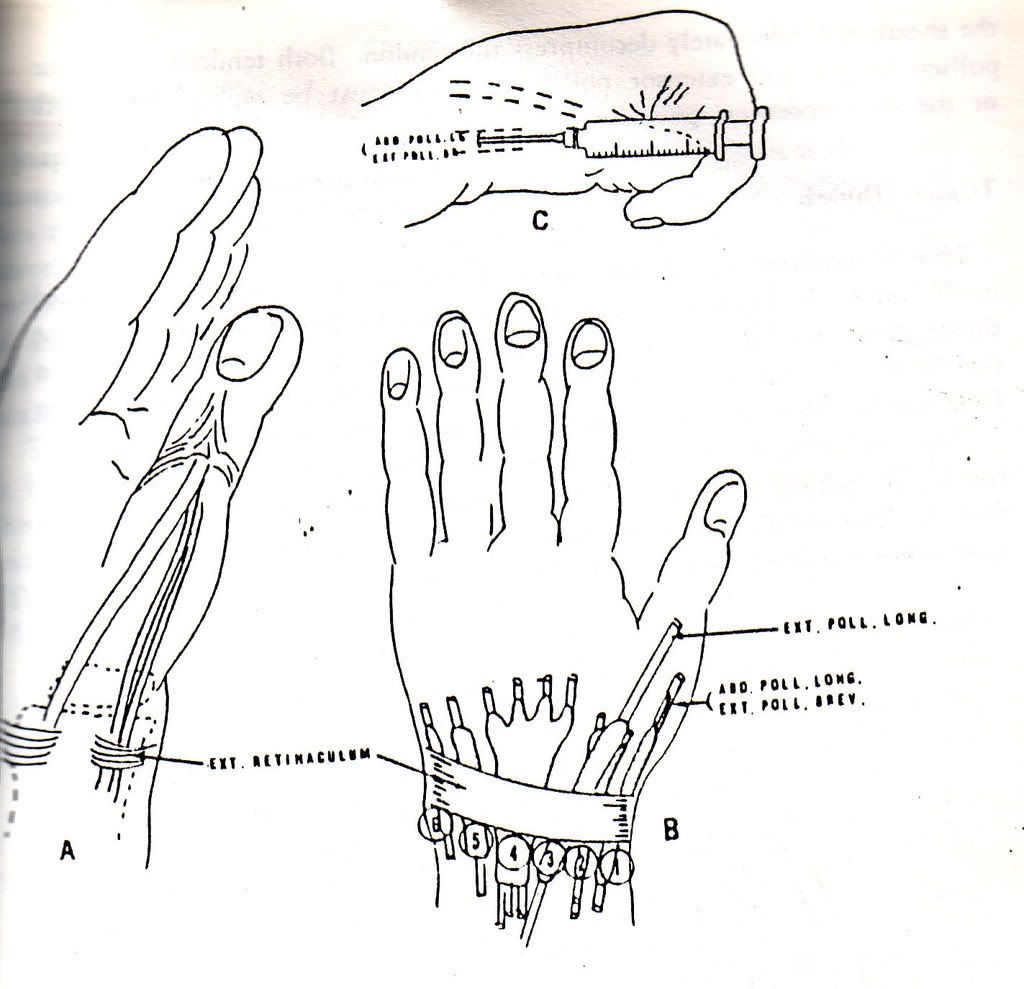
Mrs Hizkiah, a beautiful nurse, funny, always smile. 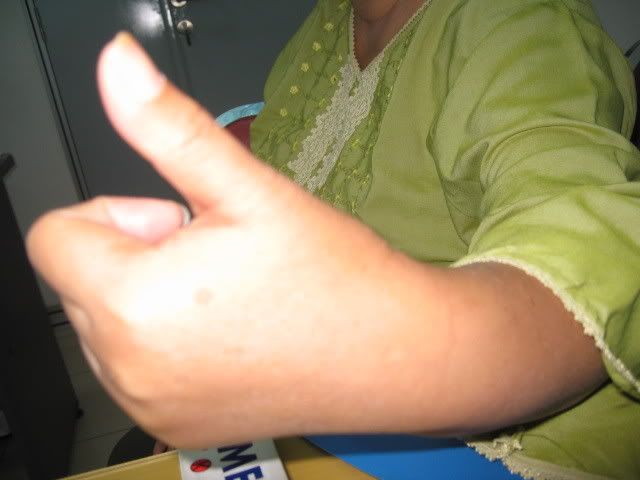 cupping it under the fingers, than flexing the wrist in an ulnar direction which streches the thumb tendons. Lovely Hizkiah, that is the reasoning, why your pain exaggerated after your therapist asked you to made a fist, forcing flex the thumb.
cupping it under the fingers, than flexing the wrist in an ulnar direction which streches the thumb tendons. Lovely Hizkiah, that is the reasoning, why your pain exaggerated after your therapist asked you to made a fist, forcing flex the thumb.