
Pingkan is in hospital now. She hospitalized due to pain on her both hands and both knees. The working diagnosis is suspect Rheumatoid Arthritis (RA) . The pain very annonying her. I promised to explain to her about RA. but I also ask her to write the history about her illness.
While waiting her story,below a highlight about RA
What is Rheumatoid arthritis (RA)
 Rheumatoid arthritis is a chronic, inflammatory, multisystem, autoimmune disorder. It is commonly polyarticular, i.e. it affects many joints. The joints are usually affected initially asymmetrically and then in a symmetrical fashion as the disease progresses. The pain generally improves with use of the affected joints, and there is usually stiffness of all joints in the morning that lasts over 1 hour. The pain of rheumatoid arthritis is usually worse in the morning.
Rheumatoid arthritis is a chronic, inflammatory, multisystem, autoimmune disorder. It is commonly polyarticular, i.e. it affects many joints. The joints are usually affected initially asymmetrically and then in a symmetrical fashion as the disease progresses. The pain generally improves with use of the affected joints, and there is usually stiffness of all joints in the morning that lasts over 1 hour. The pain of rheumatoid arthritis is usually worse in the morning.
Deformities
As the pathology progresses the inflammatory activity leads to erosion and destruction of the joint surface, which impairs their range of movement and leads to deformity. The fingers are typically deviated towards the little finger (ulnar deviation) and can assume unnatural shapes. Classical deformities in rheumatoid arthritis are the Boutonniere deformity (Hyperflexion at the proximal interphalangeal joint with hyperextension at the distal interphalangeal joint), swan neck deformity (Hyperextension at the proximal interphalangeal joint, hyperflexion at the distal interphalangeal joint). The thumb may develop a "Z-Thumb" deformity with fixed flexion and subluxation at the metacarpophalangeal joint, and hyperextension at the IP joint.

basic rehabilitation treatment principles
are:
1. relieve pain
2. prevent joint damage and eformities
3. maintain strength and function
4. educate the patient and family
5. help the patient adapt emotionally to life-style limitations
imposed by the diseases proses.
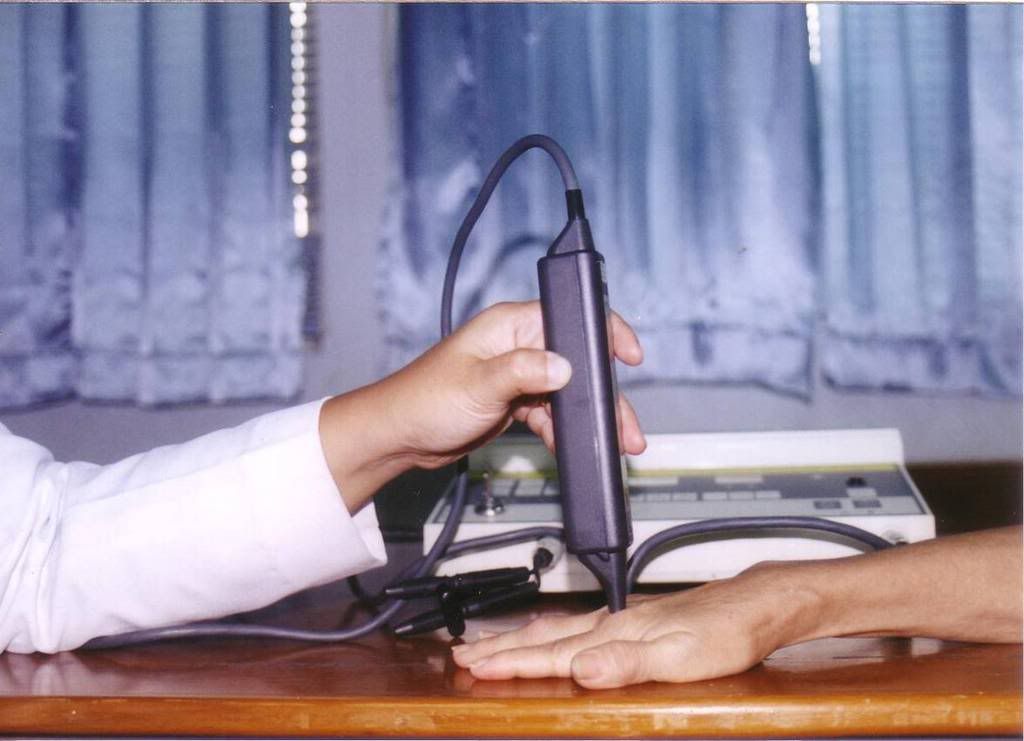
Lovely Pingkan. May be we should try to use Low Laser for you to relive pain.
Would you please click my blog about: Low Level laser in Rheumatoid Arthritis:
the paper just won the 3rd place free paper competition !
(Conclusion : Low level LASER therapy combine with isometric hand strengthening exercise can reduce pain and increase the MCP range of motions in patients with hand rheumatoid arthritis )
It is safe for you?
Phototherapy is FDA approved for a number of applications and has been deemed safe. It also requires relatively little time to perform. Established protocols and tissue dosages have been established that make clinical application relatively easy
Why you dear? Let's look the epidemiology
Epidemiology
The incidence of RA is in the region of 3 cases per 10,000 population per annum. Onset is uncommon under the age of 15 and from then on the incidence rises with age until the age of 80. The prevalence rate is 1%, with women affected three to five times as often as men. It is 4 times more common in smokers than non-smokers. Some Native American groups have higher prevalence rates (5-6%) and black persons from the Caribbean region have lower prevalence rates. First-degree relatives prevalence rate is 2-3% and disease concordance in monozygotic twins is approximately 15-20%















