
Marching brass Putri Santa Ursula
Sonya Monica dearest, this is for you
EFFECTS OF LOW POWER LASER IN FROZEN SHOULDER
Wyasa Andrianto,MD, Ferial Hadipoetro,MD,PhD, Nury Nusdwinuringtyas,MD,
Zuljasri Albar,MD,; Nyoman Murdana,MD, Suryanto Hartono,MD,MA,
Frozen shoulder :
• disorder of progressive pain and decrease of range of motion of shoulder articulation
• the main causation of shoulder pain and dysfunction in the middle and older age population
• treatment option:
• ice cooling, medicaments, exercise, TENS, ultrasound diathermy
• Low power laser therapy with exercise will decrease shoulder pain and increase the range of motion of the shoulder articulation
• improve the quality of life of patients with frozen shoulders
• Design comparison of parameter before and after therapy of frozen shoulder patients
• OPD Rehab.Med.,Rheumatology Div,Dept.Internal Med,
• December 2004 to April 2005
• Frozen shoulder patients not less than 18 years of age
• VAS not less than 8
• Cooperative
• Informed consent
• Cases with trauma of shoulder articulation
• Rheumatoid arthritis and spondyloarthritis with shoulder involvement
• Following or under corticosteroid injection therapy within the last 3 months
• Patients with abduction range of motion less than 90 degree
• patients with contraindication of laser therapy
• patients who are unable to perform shoulder exercise properly
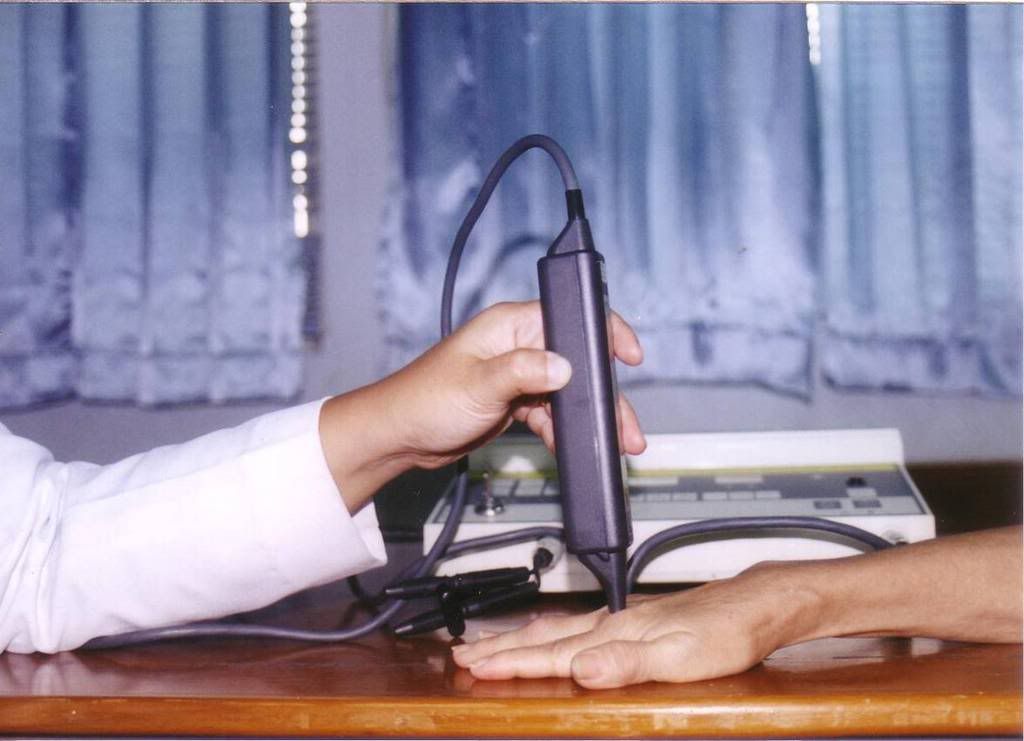
Laser device
• Endolaser 476(Enraf-Nonius)
• Wavelength : 830 nm
• Output : 30 mW
• Dose : 30 J per treatment
• Continuous wave
• 3 times per week for 3 weeks
DATA ANALYSIS
Table 1.
Group distribution of frozen shoulders
by age
| Age(year) | Total | Percentage |
| 40 – 50 51 – 60 61 – 70 | 1 2 13 | 6,25 12,5 81,25 |
Table 2.
Group distribution of frozen shoulders by sex
| Sex | Total | Percentarge |
| Male Female | 6 7 | 46,15 53,85 |
Table 3.
Group distribution of frozen shoulders
by education level
| Education level | Total | Percentage |
| Elementary School Junior High School Senior High School College University | 3 1 3 2 3 4 | 18,75 6,25 18,75 12,5 18,75 25 |
Table 4.
GROUP DISTRIBUTION OF
FROZEN SHOULDER BY PROFESSION
| PROFESSION | TOTAL | PERCENTAGE |
| PRIVATE HOUSEWIFE RETIRED/JOBLESS NURSE TEACHER | 4 6 4 1 1 | 25 37,5 25 6,25 6,25 |
Table 5.
GROUP DISTRIBUTION OF FROZEN SHOULDERS
ACCORDING TO DURATION OF SICKNESS
| DURATION | TOTAL | PERCENTAGE |
| <> ³ 2 months | 3 13 | 18,75 81,25 |
Table 6.
GROUP DISTRIBUTION OF
FROZEN SHOULDERS BY LOCATION
| Location affected | Total | Percentage |
| Left shoulder Right shoulder | 9 7 | 56,25 43,75 |
Table7.
VAS BEFORE AND AFTER TREATMENT OF
FROZEN SHOULDER
| VAS SCORE | MEAN± SD | n = 16 | p |
| VAS (pre) VAS (post) |
8,6875 ± 0,8237 1,4125 ± 0,9142 | |
0,000 |
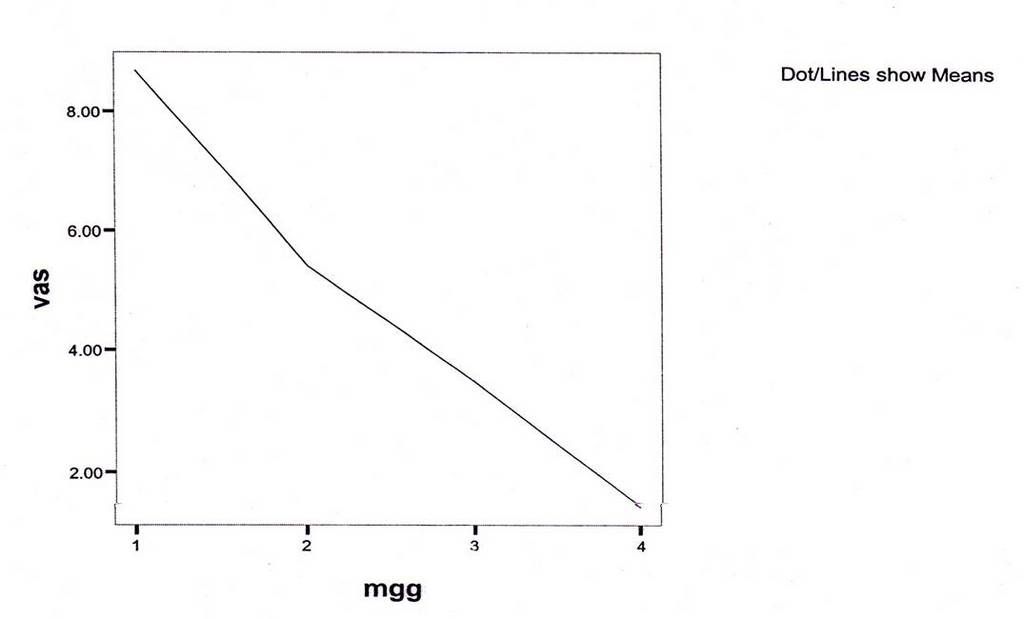
Graphic 1.
Graphic : Declining VAS score (shoulder joints)
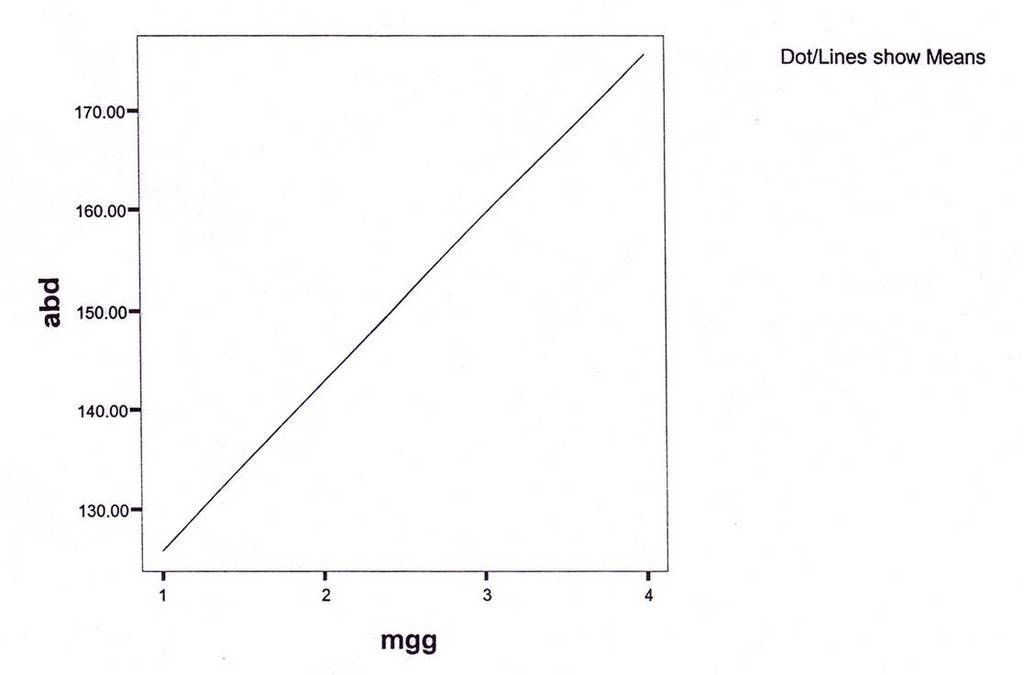
Graphic 2.
Graphic : Increasing joint movements (shoulder joints)
RESULTS AND DISCUSSION
• Significant decrement of shoulder pain before and after treatments following 3 weeks of therapy
• Significant increment of range of motion of shoulder articulations before and after treatments of low power laser therapy with shoulder exercises following 3 weeks of therapy
CONCLUSIONS
• LOW POWER LASER THERAPY AND EXERCISES OF SHOULDER ARTICULATION IS EFFECTIVE AND EFFICIENT MODALITIES TO TREAT FROZEN SHOULDER





















{kind=link}